Link Between Diabetes and Vitamin B12
M3 India Newsdesk May 11, 2024
This article comprehensively explores the association between diabetes mellitus, particularly type 2, and vitamin B12 deficiency. It outlines the mechanisms, epidemiological connections, screening approaches, and treatment strategies for managing this deficiency among diabetic patients.
Diabetes Mellitus is a chronic metabolic disorder characterised by elevated blood sugar levels (hyperglycemia) resulting from either insufficient insulin production, ineffective use of insulin, or both.
Insulin, produced by the pancreas, helps regulate blood sugar levels by facilitating the uptake of glucose into cells for energy production. When insulin function is impaired, glucose builds up in the bloodstream, leading to various complications.
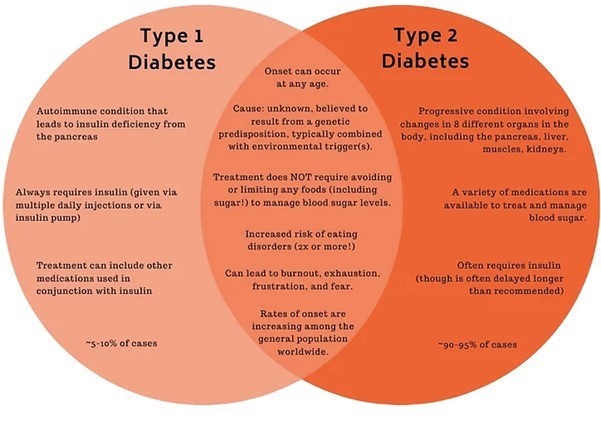
There are primarily two main types of diabetes:
The prevalence of diabetes has been steadily increasing worldwide, primarily due to factors such as ageing populations, sedentary lifestyles, unhealthy dietary habits, and rising obesity rates.
According to the International Diabetes Federation (IDF), as of 2021, approximately 537 million adults (aged 20-79) worldwide were living with diabetes, with type 2 diabetes being the most prevalent form. This number is projected to rise to 643 million by 2030 and 783 million by 2045 if current trends continue.
Vitamin B12, also known as cobalamin, is a crucial water-soluble vitamin essential for DNA synthesis, proper hematopoiesis, and neurological function. Consequently, the clinical manifestation of vitamin B12 deficiency primarily presents with haematological and neurocognitive impairments.
Role of Vitamin B12 in the body, its sources, absorption, and functions
1. Vitamin B12 exerts its physiological effects by regulating two primary enzymatic pathways:
- The methylation process of homocysteine to methionine.
- In the conversion of methylmalonyl coenzyme A (CoA) to succinyl-CoA.
2. A significant deficiency in vitamin B12 metabolism can lead to hyperhomocysteinemia, which is known to have potentially harmful effects on neurons and the vascular endothelium. This process is crucial for converting dietary folate into its active form, tetrahydrofolate. Additionally, the rise in serum methylmalonic acid (MMA) levels contributes to defective fatty acid synthesis in neuronal membranes. Vitamin B12 is also vital for neurotransmitter synthesis, including serotonin and dopamine.
3. Deficiency in vitamin B12 leads to various neurological and cognitive manifestations. Neuronal damage induced by vitamin B12 deficiency is characterised by axonal demyelination, degeneration, and eventual death, resulting in severe peripheral or autonomic neuropathy, subacute combined degeneration of the spinal cord, delirium, and dementia.
4. Vitamin B12 is an indispensable micronutrient necessary for DNA synthesis, cellular repair, and normal hematopoiesis, alongside other micronutrients such as folate and iron.
5. Deficiency is associated with haematological abnormalities such as macrocytic red blood cells, sometimes leading to anaemia, ovalocytes, hypersegmented white blood cells, and pancytopenia. Due to impaired cell repair mechanisms, atrophic glossitis, stomatitis, and malabsorption due to villi atrophy and mucositis are also prevalent.
Epidemiological connection
Several cross-sectional studies and case reports have documented an increased frequency of vitamin B12 deficiency among type 2 DM (T2DM) patients.
Metformin use has been inevitably found to be the primary aetiology for vitamin B12 deficiency among patients with T2DM.
Metformin-induced vitamin B12 deficiency among patients with T2DM
In the absence of contraindications such as renal and hepatic dysfunction, metformin is recommended as the initial treatment for lowering glucose levels, alongside lifestyle modifications.
The proposed mechanisms underlying metformin-induced vitamin B12 deficiency in patients with type 2 diabetes mellitus (T2DM) include several factors:
- Changes in small bowel motility lead to bacterial overgrowth and subsequent B12 deficiency, competitive inhibition or deactivation of B12 absorption, alterations in intrinsic factor (IF) levels, and interaction with the cubulin endocytic receptor.
- Additionally, metformin has been observed to impede the calcium-dependent absorption of the vitamin B12-IF complex in the terminal ileum. However, this inhibitory effect can be reversed with calcium supplementation.
In one early randomised controlled trial by DeFronzo et al., metformin decreased the serum vitamin B12 levels by 22% and 29% compared to placebo and glyburide respectively. The risk of developing metformin-associated vitamin B12 deficiency is greatly influenced by increasing age, metformin dose and duration of use.
Vitamin B12 deficiency among patients with type 1 diabetes mellitus
- Type 1 diabetes mellitus (T1DM) is an autoimmune disorder often accompanied by other autoimmune and endocrine conditions, leading to the development of autoimmune polyglandular syndromes.
- Pernicious anaemia, a consequence of chronic autoimmune gastritis, is highly prevalent among individuals with T1DM. Vitamin B12 deficiency resulting from pernicious anaemia is common in this patient population.
- Patients with T1DM frequently produce autoantibodies against intrinsic factor (AIF) types 1 and 2, as well as parietal cell antibodies (PCA). These PCA antibodies inhibit the secretion of intrinsic factors, leading to pernicious anaemia, a condition that occurs at a rate ten times higher among individuals with type 1 diabetes compared to those without diabetes.
- Type 1 AIF antibodies contribute to vitamin B12 deficiency by interfering with the binding of vitamin B12 to intrinsic factors, thereby hindering its transport to the absorption site in the terminal ileum. These autoantibodies are detected in approximately 70% of patients with pernicious anaemia.
- Co-occurring autoimmune hypothyroidism was found in 20.2% of 504 ambulatory T1DM patients in a cross-sectional study conducted in South Africa. This frequency was higher in female patients (30.9% vs.10.1 %-males, p<0.0002). Celiac disease in this study cohort was reported in 3 (0.6%) patients.
- Primary autoimmune hypothyroidism and celiac disease are frequent co-morbidities among patients with T1DM and directly affect vitamin B12 metabolism.
Screening approach for vitamin B12 deficiency among patients with T2DM
Currently, there are no established guidelines recommending routine screening for vitamin B12 deficiency in individuals with type 2 diabetes mellitus (T2DM). However, it is clinically reasonable to consider screening for vitamin B12 deficiency in type 2 diabetic patients before starting metformin treatment.
Subsequently, screening annually may be warranted, particularly in elderly patients with a history of prolonged metformin use (≥3-4 years), those on high doses of metformin (≥2 g/day), or those experiencing worsening diabetic distal polyneuropathy, regardless of the presence or absence of haematological abnormalities discussed earlier.
The initial screening step for vitamin B12 deficiency in individuals with T2DM should involve measuring serum vitamin B12 concentrations. Levels below 200 pg/ml are typically indicative of vitamin B12 deficiency.
For individuals with borderline serum vitamin B12 concentrations (200-400 pg/ml) and subtle haematological manifestations, a more sensitive and specific approach involves measuring serum methylmalonic acid (MMA) or homocysteine concentrations.
In the case of type 1 diabetes mellitus (T1DM), due to the notable prevalence of pernicious anaemia and subsequent vitamin B12 deficiency among T1DM patients as reported in various cross-sectional studies, it may be prudent to screen at the time of diagnosis and subsequently on an annual basis for the first three years.
Afterwards, screening every five years or when clinically indicated is advisable since vitamin B12 deficiency can arise at any time. Screening should encompass assessing serum vitamin B12 levels and markers of gastric autoimmunity such as parietal cell antibodies (PCA) and intrinsic factor antibodies (AIF), particularly in T1DM patients with glutamic acid decarboxylase 65 antibodies (GAD-65) and thyroid peroxidase antibodies.
Treatment of vitamin B12 deficiency among diabetic patients
- All patients with a deficiency of vitamin B12 should undergo replacement therapy, either orally or parenterally. For adult patients with type 2 diabetes mellitus (T2DM), intramuscular or oral administration of vitamin B12 at doses of 1000 μg daily for one week, followed by once-weekly dosing for four weeks, is considered adequate to correct the deficiency.
- In young patients with type 1 diabetes mellitus (T1DM) who also have a vitamin B12 deficiency, replacement therapy involves daily intramuscular or oral administration of vitamin B12 at a dose of 100 μg for one week, followed by monthly dosing.
- Severe cases may necessitate parenteral or oral administration of 1000 μg/day of vitamin B12 for one week, followed by weekly dosing for one month, and then monthly thereafter.
- If there is concurrent folate deficiency, oral folate replacement therapy at doses of 5 mg daily for 1–4 months is recommended. However, administering folate before correcting the vitamin B12 deficiency should be avoided, as it can exacerbate or worsen the associated neurological manifestations.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr. Akshayaa is a General Practitioner at Sri. Balaji Heart Centre, Chennai.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
