RA and Cardiovascular Health: Exploring the Link
M3 India Newsdesk Jun 05, 2023
Rheumatoid arthritis (RA) and cardiovascular health are closely linked. In this article, the author has delved into the complex relationship between rheumatoid arthritis and cardiovascular disease, highlighting the underlying mechanisms, shared risk factors, and implications for clinical management.
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease primarily known for its effects on the joints. However, it is a systemic disease which can impact other organ systems. The leading cause of mortality in these patients is also premature atherosclerotic cardiovascular disease comparable to patients with diabetes mellitus.
Understanding the connection between RA and CVD
Multiple epidemiological studies have consistently demonstrated a 1.5 to 2-fold higher incidence of myocardial infarction, stroke, and overall cardiovascular mortality compared to the general population in RA patients. These patients are more likely to have silent ischemic heart disease, develop heart failure, and experience sudden death.
This excess CV risk is closely linked to RA disease severity and chronic inflammation, hence is largely underestimated by traditional risk calculators such as the Framingham Risk Score, the Reynolds Risk Score (RSS), or the Systemic Coronary Risk Evaluation (SCORE).
Patients have a higher atherosclerotic burden, with up to a 2.5-fold increase in coronary artery calcifications (CAC) measured by cardiac computed tomography (CT) and CT angiography.
Shared risk factors
Several risk factors are shared between rheumatoid arthritis and cardiovascular disease.
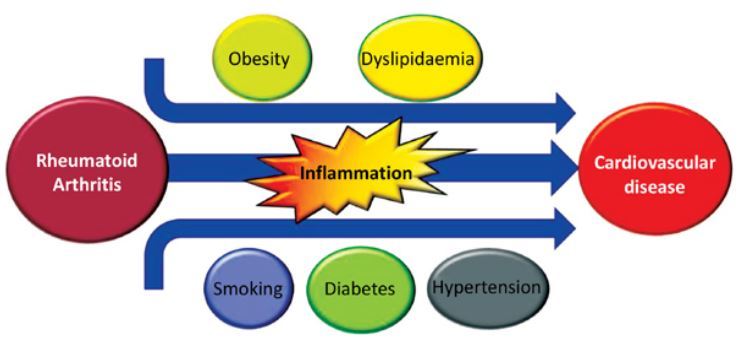
- Chronic systemic inflammation, involving both the innate and the adaptive immune system, exerts direct and indirect effects on the vasculature and myocardium, with mechanistic evidence implicating elevated acute phase reactants, pro-inflammatory cytokines, autoantibodies, and specific T-cell subsets.
- Additionally, traditional risk factors such as Smoking, Hypertension, Dyslipidemia, Diabetes mellitus, Obesity, Functional impairment, and Steroid & NSAID usage, are often prevalent in patients with RA which further increases the risk of cardiovascular events.
Inflammatory pathways
The chronic systemic inflammation characteristic of rheumatoid arthritis may directly promote atherosclerosis and endothelial dysfunction.
1. Inflammatory burden:
- Inflammatory cytokines: Including tumour necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and interleukin-1 (IL-1), can accelerate the progression of atherosclerotic plaques and contribute to the instability of these plaques, increasing the risk of cardiovascular events.
- Autoantibodies: The presence of anti-citrullinated peptide antibodies (ACPAs), anti-malondialdehyde-acetaldehyde adducts (anti-MAA), and anti-carbamylated proteins (anti-CarP) antibodies have been associated with an increased risk of CV death in RA patients by potentially promoting atherosclerotic plaque formation and cardiac remodelling.
2. Endothelial Dysfunction:
Endothelial dysfunction, a key event in atherosclerosis development, is prevalent in patients with rheumatoid arthritis. Inflammation-induced oxidative stress, impaired nitric oxide (NO) production and increased endothelial cell activation are some of the mechanisms leading to endothelial dysfunction. This dysfunction leads to impaired vasodilation, a prothrombotic state, and increased vascular permeability, further promoting atherosclerosis and CVD.
Effects of RA treatments on cardiovascular health
- Several studies have explored the impact of disease-modifying anti-rheumatic drugs (DMARDs) and biological agents on cardiovascular risk in RA patients.
- Some DMARDs, such as methotrexate, have shown potential cardiovascular benefits by reducing systemic inflammation and improving endothelial function.
- Biologic agents targeting specific inflammatory pathways, such as TNF inhibitors, abatacept and rituximab have also demonstrated favourable effects on cardiovascular outcomes in RA patients.
- But frequently used medications for symptomatic treatment in patients with RA like NSAIDs and Glucocorticoids may have dose-dependent ill effects on CV-related morbidity.
- Concerns with JAK inhibitors and Anti IL 6 Monoclonal antibody: Both can increase LDL and total cholesterol by 10-20% which remains a concern for CV morbidity.
- Data from Oral Surveillance trials remains a concern for JAK inhibitors and CV safety, especially in patients with underlying additional CV risk factors.
Clinical implications
Given the substantial cardiovascular risk associated with rheumatoid arthritis, recent guidelines for the management of RA are encouraging rheumatologists to assess and coordinate CVD risk management in such patients. Although optimal guidelines and assessment tools are scarce; aggressive control of disease activity, monitoring and treating traditional risk factors, promoting a healthy lifestyle, and considering cardiovascular risk when selecting appropriate treatment strategies can help mitigate CV risk.
Multidisciplinary collaboration between rheumatologists and cardiologists is crucial to optimise patient care and minimise cardiovascular morbidity and mortality. It includes patient education and awareness, comprehensive assessment, speciality management, and optimal and monitored treatment.
Key notes
- Patients with RA have a higher risk of developing cardiovascular disease (CVD), including heart attacks and strokes.
- Shared risk factors such as chronic inflammation, smoking, hypertension, dyslipidemia, obesity, and a sedentary lifestyle contribute to this increased risk.
- Inflammatory pathways and endothelial dysfunction play key roles in promoting atherosclerosis and cardiovascular events in RA patients.
- Effective management of RA, including disease-modifying anti-rheumatic drugs (DMARDs) and biological agents, can help reduce inflammation and improve cardiovascular outcomes whereas glucocorticoids and NSAIDS may have dose-dependent ill effects on CV-related morbidity.
- Comprehensive assessment and treatment of cardiovascular risk factors, along with multidisciplinary care, are crucial to minimising cardiovascular morbidity and mortality in RA patients.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Naman Jain is a consultant rheumatologist at Ramkrishna Care Hospital Raipur, Chattisgarh.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
