Chronic Knee Discomfort Diagnosis: JAMA Updates
M3 India Newsdesk Feb 07, 2024
This comprehensive article on knee discomfort explores the increasing prevalence of knee issues, emphasising on the crucial role of a thorough assessment by practitioners.
Approximately 25% of persons have knee discomfort, which has grown by approximately 65% in the last 20 years and accounts for over 4 million primary care visits each year. The first assessment should concentrate on ruling out urgent reasons and taking referral requirements into account. To differentiate the diagnosis, a thorough, standardised history and physical examination are essential.
Nonsurgical issues don't always need a quick, conclusive diagnosis, and when necessary, imaging and lab tests may serve as confirmatory or diagnostic measures.
Implications for non-orthopaedic doctors
Research indicates that a significant number of non-orthopedic doctors are unconfident while doing clinical musculoskeletal exams, and 78–82% of recently graduated medical students are unable to demonstrate basic ability.
The "Rules of Four" approach, a methodical knee examination technique is presented in this article to assist non-orthopaedic clinicians in confidently reaching a workable diagnosis when assessing a patient's knee complaint. The method separates the knee into three columns, each including four examination locations, and a fourth column that contains the four major knee ligaments.
1. Before sending a patient to an orthopaedic surgeon, this technique enables doctors to rapidly and correctly arrive at a working diagnosis. Based on that diagnosis, suggestions for further treatments, such as therapy, injections, bracing, rest, activity adjustment, or direct imaging, may be made.
2. Three columns—medial, central, and lateral—each with four test points—make up the knee exam.
Common causes of knee discomfort include:
- Tears in the medial meniscus
- Medial collateral ligament (MCL)
- Medial patellofemoral ligament/reticulum (MPFL)
- Pes anserine bursitis
These injuries occur in the medial column. Consideration should also be given to a medial tibial plateau fracture if there has been a history of substantial knee trauma recently.
- The medial femoral condyle, the site of the medial collateral ligament's origin, should be felt initially. Tenderness to palpation above the medial femoral condyle may be indicative of an MCL tear or avulsion.
- The second aspect concerns the medial patellofemoral ligament (MPFL), which might tear when a patient has lateral patellar dislocation due to patellar instability. When combined with patellar instability, tenderness to palpation over the MPFL is regarded as a positive test and suggests a tear in the MPFL.
- The third point is the medial joint line, which often denotes the medial meniscal tear and degenerative joint disease, two prevalent aetiologies. Two frequent aetiologies of tenderness to palpation along the medial joint line are degenerative joint disease and medial meniscal tears.
- The pes anserine bursa is the fourth and last point. It may be palpated somewhat inferior and two-finger breaths medial to the tibial tubercle, or it can be observably enlarged.
3. Common causes of knee discomfort from the middle column are:
- Quadriceps tendon rupture
- Tendinitis
- Patellar fracture
- Prepatellar bursitis
- Patellofemoral pain syndrome
- Patellar tendinitis
- Sinding-Larsen-Johansson syndrome
- Osgood-Schlatter disease
Many conditions may lead to knee discomfort that originates in the lateral column of the knee such as:
- Patellar instability
- Degenerative joint disease
- Proximal fibula fracture
- Lateral meniscal tear
- Proximal tibiofibular dislocation
4. IT band syndrome
IT band syndrome is characterised by tenderness on palpation at the location where the IT band passes across the lateral femoral epicondyle.
The patient may be instructed to lay on their contralateral side and range from extension to flexion if a negative assessment is detected. Another thing to look for is the patellar apprehension test for patellar instability.
Two possible aetiologies of tenderness to palpation along the lateral joint line are degenerative joint disease and lateral meniscal tears. The tibia is internally rotated, and the knee is moved into extension while feeling the lateral joint line for a painful, audible click if the discomfort is not relieved.
Radiographs may confirm the diagnosis of meniscal tear and degenerative joint disease, respectively, and may be followed by an MRI.
Ligament injury
The four main knee ligaments whose stability is evaluated are :
-
The anterior cruciate ligament (ACL)
- Posterior cruciate ligament (PCL)
- Medial collateral ligament (MCL)
- Lateral collateral ligament (LCL)
An accurate diagnosis of ligamentous injuries requires a comparison with the contralateral side that is undamaged. Because it causes less discomfort for the patient and lessens the impact of protective muscle contraction, the Lachman test is the most reliable method for detecting ACL rupture in both acute and chronic injuries.
The tibia stays anterior to the femoral condyles during a posterior drawer test, which evaluates the integrity of the PCL. The PCL is probably ruptured if the tibia is translated flush with the femoral condyles.
A valgus stress test is used to examine the MCL when the knee is at 30 degrees of flexion to isolate the ligament. Increased medial gapping or the absence of a solid terminus are signs of MCL damage.
The varus stress test is used to assess the LCL. The Rules of Four technique is a methodical way that non-orthopaedic doctors may use to assess a patient's knee complaint. It facilitates the prompt identification of common musculoskeletal ailments and guides further testing and treatment.
In conclusion, physical examination techniques are essential for determining the cause and course of therapy for knee problems.
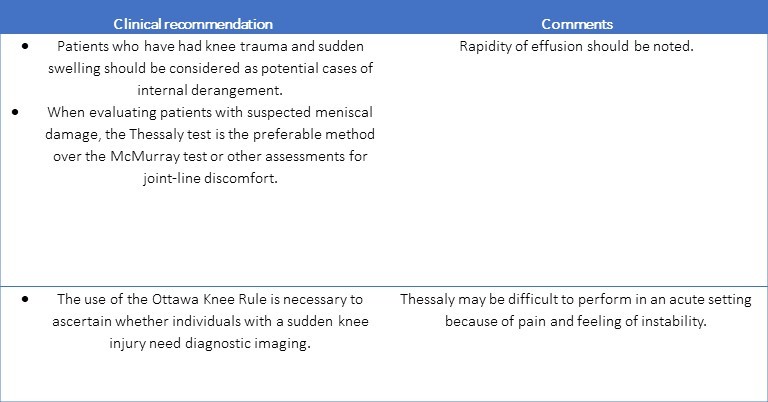
The foundation of the first assessment for acute knee injury is a thorough history and physical examination. Thessaly testing—which is favoured over the McMurray test—as well as the Valgus and Varus stress tests are the most often used methods for evaluating meniscal injuries.
These tests assess for posterior collateral ligament (PCL) damage; in 20 out of 24 patients, the sag sign accurately diagnoses PCL injury, and in 18 out of 24 patients, "quad activation" correctly diagnoses PCL injury.
Radiography
Radiography should only be used for acute traumatic pain in individuals who fulfil certain evidence-based criteria or for persistent knee pain lasting more than six weeks to further examine undifferentiated knee pain.
Imaging judgements are supported by the Ottawa Knee Rule, Pittsburgh Knee Rule, and American College of Radiology Appropriateness Criteria. Anteroposterior, lateral, and Merchant's views are the three radiographic views that are advised (for the patellofemoral joint).
Osteochondral lesions may be seen with the notch or tunnel view, whereas oblique views can be used to check for tibial plateau fractures. Weight-bearing radiographs should be taken to check for joint-space narrowing, subchondral sclerosis, osteophytes, and bony cysts if osteoarthritis is suspected.
A qualified clinician's use of musculoskeletal ultrasonography permits limited assessment of muscles, vasculature, nerves, superficial tendons, cysts, and effusions.
Via the use of an ultrasonic transducer, mechanical symptoms like snapping, clicking, or popping may be palpated and assessed. Rarely is an emergent MRI necessary; instead, it is usually saved for surgical reasons that may arise, such as dislocation, a tear of the ACL or PCL, a fracture that is not obvious on radiography, a rupture in the vertical meniscus, cancer, vascular damage, or osteomyelitis. An MRI should ideally support the results of the physical examination and history.
When the initial history and physical examination point towards a diagnosis but are unable to definitively confirm it, a laboratory investigation may be helpful in both confirmatory and diagnostic roles. Serology for autoimmune disorders and suspected inflammatory illnesses, as well as microscopic analysis of arthrocentesis fluid for bacterial infection or gouty crystals, might all be part of this workup.
Prompt steps
- Any knee discomfort that raises the possibility of a serious acute traumatic injury (fracture, dislocation), has to be evaluated and treated every once.
- Knee pain that raises the possibility of infection is an emergency that has to be treated right away. A specialist (often an orthopaedic surgeon or emergency care physician) should be consulted for advice on diagnosis and treatment.
Key points
- A common musculoskeletal ailment that affects around 25% of individuals is knee discomfort.
- The majority of the pain is localised in the knee joint and is brought on by intrinsic or referred problems.
- The clinical history of the patient, which includes information on age, comorbid diseases, activities, pain location, symptoms of mechanical joints, joint effusion, and soreness, is used to make the diagnosis.
- The first stage is to rule out diagnoses that need immediate attention.
- The first imaging study of choice is radiography; advanced imaging is reserved for chronic discomfort and preoperative assessment.
- In some clinical situations, laboratory tests may be utilised as a confirmatory or diagnostic measure.
- Arthrocentesis is recommended for infected joints and can be necessary to verify arthritis caused by crystals.
Potential concerns
- When there is a high likelihood that imaging will have an impact on care, it is important to order imaging.
- If a patient has anterior knee pain but no mechanical symptoms or effusion, it is not necessary to order a knee MRI unless the patient has not improved after completing a suitable functional rehabilitation programme.
- Failure to evaluate for disease involving the nearby joints and anatomic regions (e.g., hip, lumbar spine) may result in missed diagnosis of conditions associated with referred pain to the knee.
Key recommendations for practice
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Monish Raut is a practising super specialist from New Delhi.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
