Should I give chloroquine/hydroxychloroquine for prevention of COVID-19?: Dr. Sundeep Mishra
M3 India Newsdesk Jul 10, 2020
Dr. Sundeep Mishra answers questions on prescribing two medications- chloroquine and hydroxychloroquine, currently being used as prophylactic therapies in the fight against COVID-19.
For our comprehensive coverage and latest updates on COVID-19 click here.
Prevention of COVID-19 - Part 1
COVID-19 is a viral infection and thus follows all the rules and properties of a viral infection. All viruses are pathogens and some infect humans but most are controlled satisfactorily by the human immune system with limited damage to host tissues. However, some viruses like the one causing COVID-19, may cause extensive damage to the host- in some cases, either as a viral damage, but more commonly as a consequence of adaptive immune response.
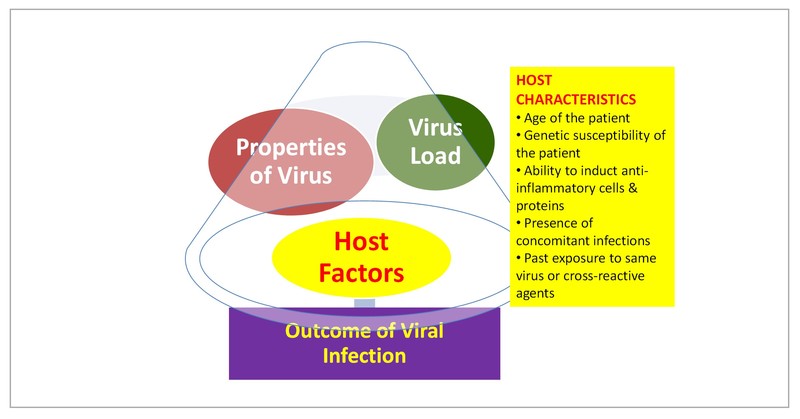
As a matter of fact, after any viral infection the outcome is dependent on three factors:
- The properties of the infecting virus (in this case SARS-CoV-2)
- The circumstance of viral infection (dose and route of infection)
- Several host factors which include- age of the host, genetic susceptibility, ability to induct anti-inflammatory cells and proteins, presence of concomitant infections and past exposure to same virus or cross-reactive agents
Factors affecting outcomes of a viral infection
Most instances of viral infections are resolved with or without tissue damage and even re-infections are usually subclinical. However with some viral infections such as HIV, hepatitis C virus (HCV), hepatitis B virus (HBV) or COVID-19, substantial tissue damage can be caused in some or all patients they infect. These viruses usually have ≥1 properties that allow them to diminish the efficacy of host innate or adaptive immunity.
In the term COVID-19 ‘CO’ stands for corona (referring to crown shape), ‘VI’ for virus, ‘D’ for disease and 19 from the year this zoonotic disease (disease of animals) became first transmitted to humans. In itself COVID-19 is not a very deadly disease causing mortality in ~5% unlike Ebola virus where mortality is >50% but it is at least 10 times more deadly than seasonal flu (mortality 0.1%).
However, the special feature about COVID-19 is its infectivity. As a virus it is similar to SARS, and that is why it is officially called SARS-CoV-2. It even attaches to the same receptors as SARS-CoV-1, but it is much more stickier (infective); the virus enters cells of the respiratory tract more quickly, gets a firmer grasp, multiplies there and starts spreading more quickly throughout the body. It can infect both nasopharynx, upper respiratory tract and lower respiratory tract (the bronchial tree and the lungs). It multiplies logarithmically in these regions and then infects the rest of the body. This triggers an inflammatory response as the body attempts to fight the invader but in ~15%, there could be an immunological over-reaction in various organs infected and may even cause a cytokine storm. This over-reaction is more harmful then beneficial and is the cause for most morbidity and mortality.
How can we prevent this virus from causing disease?
COVID-19 vaccine is not yet available and the virus is not affected by any antibiotic (antibiotics only act on bacteria or fungus and not virus). The disease can be impacted by any of the 3 factors affecting outcome. Properties of the infecting virus keep on changing depending on the genetic strain but they cannot be generally altered by human intervention but the way the virus infects can be possibly altered by some drugs like chloroquine/hydroxychloroquine (CQ/HCQ).
On the other hand, load of the virus can significantly be impacted by several lifestyle measures like social isolation, wearing masks, frequently cleaning hands, and doing steam inhalation and throat gargle. Most host factors like age, genetic susceptibility, past exposure cannot be altered, but host immune response may be modified by various lifestyle measures and some therapeutic agents.
Chloroquine and Hydroxychloroquine
What is the mechanism of effect & current status in prevention?
Both CQ & its derivative molecule HCQ act via altering the viral receptor- angiotensin converting enzyme 2 (ACE2) receptor which is the site through which COVID-19 enters the cell. They impair the terminal glycosylation of the ACE2 receptor, the binding site for the envelope spike glycoprotein of the virus. In addition, they inhibits the endo-lysosome function amd reduce viral proliferation, together with the advantages of immune-modulatory activity. Thus, these drugs may decrease the infectivity of the virus to human cells and therefore are of potential use as prophylactic and therapeutic agents.
Evidence of action
In the lab, Both CQ and HCQ have been shown to prevent the growth of the virus that causes COVID-19. In those exposed to COVID-19, use of these drugs has been shown to result in faster nasopharyngeal viral clearance. There are a few reports of patients with COVID-19 who received these drugs and improved. An American RCT of HCQ in post-exposure subjects revealed numerical benefits in reducing the risk of COVID infection although not statistically significant. However, it is not known whether it was the drug that is useful or some other factors.
In addition, the drugs in daily dose (higher doses) may produce certain side effects- including QT prolongation on ECG. Some investigators have proposed a much lower dose- weekly instead of daily and thus the side-effects are remarkably less (practically nil) with this dosing strategy.
In a study conducted in healthcare workers possibly exposed to COVID-19, sponsored by the Indian Council of Medical Research (ICMR), weekly use of HCQ for ≥4 weeks was associated with a significant decline of COVID-19 infection and in those receiving Rx for ≥6 weeks, an 80% decrease in the odds of COVID-19 infection among the healthcare workers. Thus, the Ministry of Health recommends it in prophylaxis of those individuals at high-risk of developing COVID infections.
Which drug to use: Chloroquine or hydroxychloroquine?
Hydroxychloroquine seems to have a greater (in vitro) activity against SARS-CoV-2 than CQ. Not only is HCQ more effective but it has much lesser toxicity compared to CQ and thus is much safer (retinal toxicity).
Dosage in prophylaxis
- Health workers exposed to COVID-19: HCQ 400 mg twice a day on day 1, followed by 400 mg once a week for the next 7 weeks, to be taken with meals.
- High-risk Individuals exposed to COVID-19 (elderly, immunocompromised): HCQ 400 mg twice a day on day 1, followed by 400 mg, once a week for the next 5 weeks, to be taken with meals.
- Asymptomatic contacts/suspected contacts to COVID-19: HCQ 400 mg twice a day on day 1, followed by 400 mg, once a week for the next 3 weeks, to be taken with meals.
Side effects and contraindications
In the doses recommended for prophylaxis, HCQ is very safe with the exception of occasional rashes or other side effects. However, it may be prudent to be careful in those patients who are known cases of long QT syndrome or those on macrolide antibiotics like erythromycin, azithromycin or clarithromycin. In patients <15 years of age, HCQ is contraindicated.
To read other articles by Dr. Mishra, click here.
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The writer, Dr. Sundeep Mishra is a Professor of Cardiology.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
