Optimising Caesarean Section Practices
M3 India Newsdesk Mar 03, 2025
The rising caesarean rates are a major public health problem and this needs to be addressed through evidence-based guidance. Optimising caesarean section rates is an important component.
Caesarean section is the most commonly performed surgical procedure in the world. Caesarean section when clinically indicated is a life-saving procedure for both mother and child. The term ‘optimising caesarean practices’ means ensuring the best possible use of caesarean section so that it leads to the improvement of maternal and newborn health. This means that the caesarean section is done when indicated.
The caesarean section rates have been rising. The global caesarean section rate increased from 6.7% to 19% from 1994 to 2014, a 12.4% rise. India is witnessing a similar trend with the caesarean section rate being just 3% in 1992-93. It has increased to 17% in 2015-16 and 21% in 2020-21.
Factors influencing the rate of caesarean section CS
Several factors have an impact on the rates of caesarean section. It includes:
- Age of marriage
- Age of delivery
- Presence of co-morbidities
- High-risk factors like diabetes, hypertension, obesity, heart diseases
- Birth order
- Baby weight
- Any factor hampering foetal well-being
- Mother's education level
- Socioeconomic status
- Exposure to media
- Apprehension regarding pain associated with vaginal delivery
- Belief in delivery at an auspicious time
The place of delivery whether in a rural or urban area, public sector or private sector, also influences the caesarean section rates.
We need to ensure that caesarean section is available, affordable and accessible when needed by the mother and her baby. However, consent and care should be provided with respect and dignity.
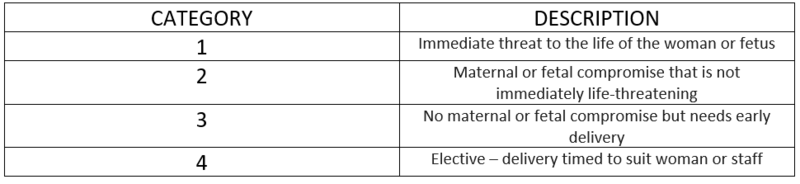
Indication of caesarean
The indication of caesarean section has been divided into 4 categories depending on the urgency and threat to the life of both the woman and foetus.
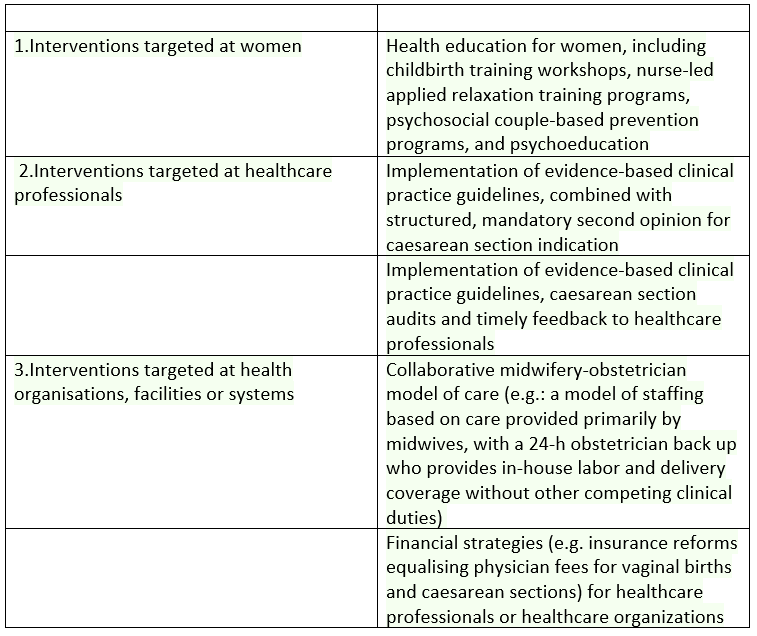
The WHO has published evidence-based recommendations on non-clinical interventions to reduce unnecessary CS. Evidence was derived from an updated Cochrane review of 29 studies.
However, FOGSI defers from having a specific caesarean section rate for any country. In 1985 WHO stated that it is not justified for any region to have a CS rate of more than 10-15 %. However, in 2015 it gave a new statement that the aim should be to provide CS to a woman in need rather than to maintain a certain rate.
The studies that WHO used for the 15% CS rate were incomplete, relying on average CS rates from multiple years rather than year-to-year variations.WHO document focused on mortality rather than morbidity. It also did not consider the long-term effects of VD like pelvic organ prolapse, sphincter injury, sexual dysfunction, fistula, urinary incontinence, etc.
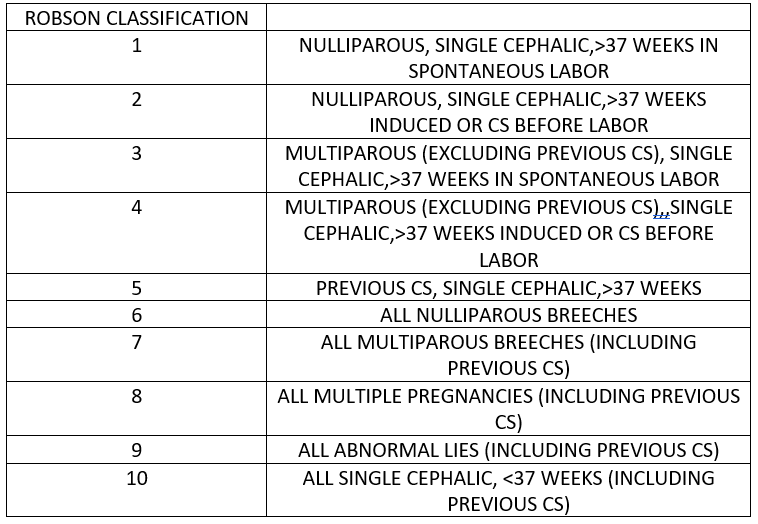
ROBSON’s ten-group classification
FOGSI states that a registry should be maintained where anonymous data at the hospital level is collected using WHO-recommended ROBSON’s ten-group classification.
Our aim should be to ensure individualised care for labouring women to ensure safe and successful vaginal delivery with the ability to perform CS to reduce maternal and perinatal mortality and morbidity.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Nancy Jena is a PG Resident (Obstetrics & Gynaecology) from Bhubaneshwar, Odisha.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
