Hydrochlorothiazide for Recurrent Renal Stone
M3 India Newsdesk Jun 19, 2023
Kidney stones recur frequently, and they cause enormous healthcare expenditures and excess illness. The article discusses the mechanism of action, potential side effects, & shortcomings of earlier research when it comes to the use of thiazide diuretics for preventing kidney stone recurrence.
Most kidney stones are composed of calcium oxalate, calcium phosphate, or a mixture of these components; indeed, hypercalciuria is the most common metabolic abnormality among patients with kidney stones. Thiazide and Thiazide-like diuretic agents (collectively referred to as Thiazide) have been the cornerstone of pharmacologic prevention of recurrence for more than 50 years.
It is important to understand the etiopathology behind stone formation to understand the treatment and the basis for the use of thiazide diuretics.
Aetiology and pathophysiology of renal stone formation
Urolithiasis may occur due to the following:
- Anatomic features leading to urinary stasis
- Low urine volume
- Dietary factors (e.g., high oxalate or high sodium)
- Urinary tract infections
- Systemic acidosis
- Medications (e.g. Sulfonamides)
- Genetic factors such as cystinuria
The most common cause of stone disease is inadequate hydration and subsequent low urine volume.
The other four most common factors contributing to urinary stone formation are:
- Hypercalciuria
- Hyperoxaluria
- Hyperuricosuria
- Hypocitraturia
Pathophysiology
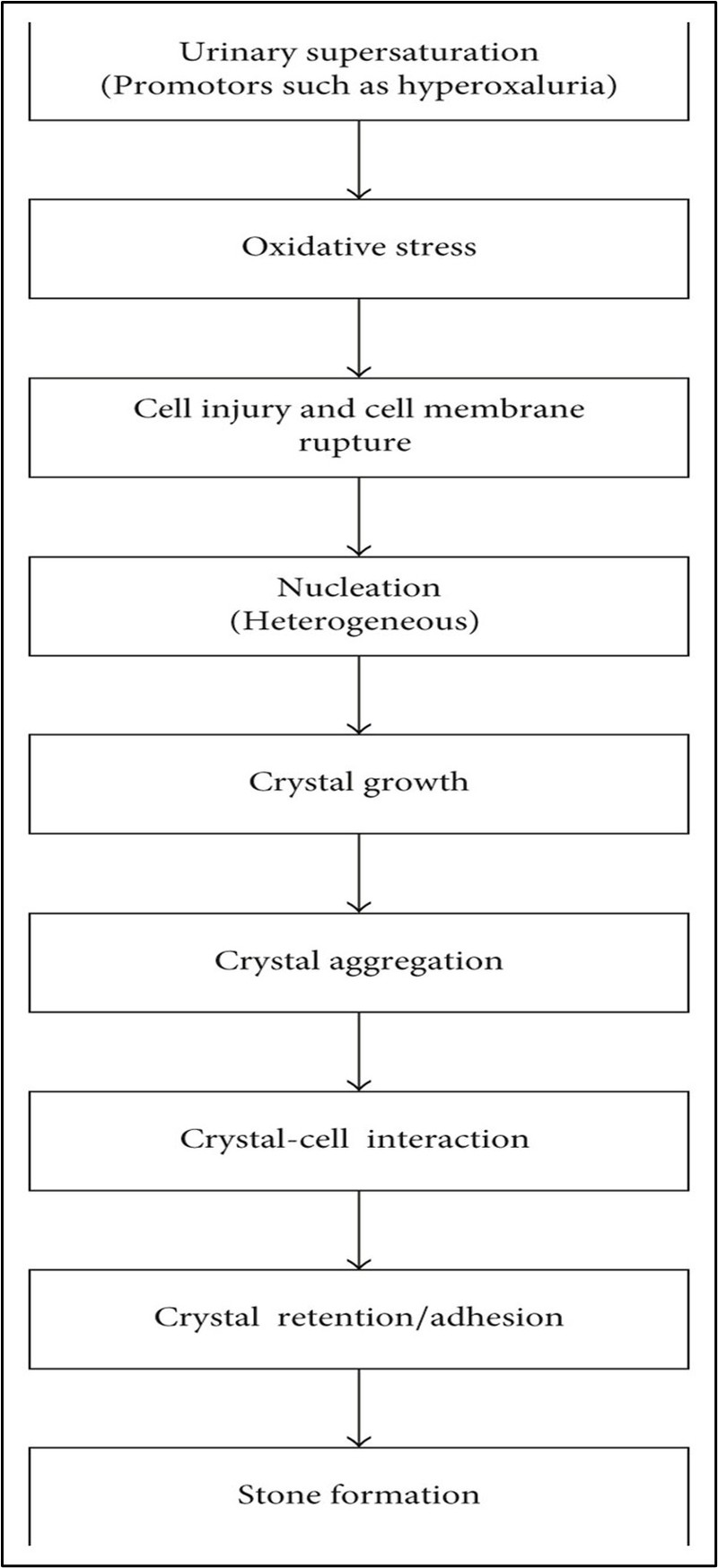
Types of renal stone
The four major types of renal calculi include:
- Calcium stones (due to hyperparathyroidism, renal calcium leak, Hyperoxaluria, hypomagnesaemia, and Hypocitraturia).
- Uric acid stones are associated with a pH of less than 5, a high intake of purine foods (fish, legumes, meat), or cancer. These stones may also be associated with gout.
- Struvite stones (caused by gram-negative-urease positive organisms that breakdown urea into ammonia. Common organisms include pseudomonas, proteus, and Klebsiella. E coli is not associated with struvite stones).
- Cystine stones are due to an intrinsic metabolic defect causing the failure of the renal tubules to reabsorb cystine, lysine, ornithine, and arginine.
Hydrochlorothiazide
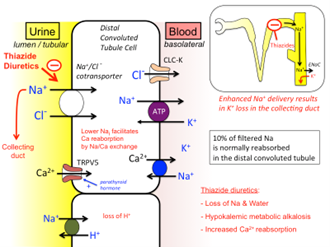
1. Mechanism of action
- Thiazides are secreted in proximal tubules and act intraluminally by inhibiting Na/Cl symporter in Distal convoluted tubules.
- They enhance Ca reabsorption in the distal convoluted tubule, by increasing Na/Ca exchange and thus reduce the urinary excretion of calcium.
- Due to increased distal Na delivery, there is an increase in aldosterone-mediated K and H ions excretion causing lower urinary pH.
Mechanism of action
2. The rationale for the use
Thiazide acts in two ways to reduce calcium oxalate stones:
- Decreases Urinary ph and thus lowers calcium phosphate supersaturation.
- Decreasing urinary calcium and thus reducing calcium oxalate supersaturation.
3. Potential adverse effects
- Hypokalemic metabolic alkalosis
- Hyponatremia
- Hyperuricemia
- Hyperglycemia
- Dyslipidemia
4. Trials and studies supporting its use
Many older studies in the last 5 decades have concluded that thiazide diuretics like hydrochlorothiazide help in reducing the recurrence of calcium stones.
- Limitations of older studies
- Inadequate concealment of treatment assignment
- A lack of double-blinding
- A lack of an intention-to-treat analysis
- The use of outdated dietary recommendation
- The use of imaging methods with low sensitivity and specificity.
- Also, only high doses of thiazides were studied; such dose levels are known to increase the risk of adverse effects
Thus, both the efficacy of thiazides in the prevention of the recurrence of kidney stones and the dose-response effect remain unclear
5. Recent trial
- NOSTONE trial, a double-blind, randomised, placebo-controlled trial was conducted to evaluate a range of hydrochlorothiazide doses for the prevention of the recurrence of kidney stones.
- A large trial of 416 patients followed over 2.9 years was conducted by Nasser A. Dhayat and colleagues which was published on 2nd March 2023 in The NEJM.
- Among patients with recurrent kidney stones, the incidence of recurrence did not appear to differ substantially among patients receiving hydrochlorothiazide once daily at a dose of 12.5 mg, 25 mg, or 50 mg or placebo once daily.
- There was a reduction in rates of radiologic stone recurrence in patients receiving higher doses of hydrochlorothiazide but was not statistically significant.
- New-onset diabetes mellitus, hypokalemia, gout, skin allergy, and a plasma creatinine level exceeding 150% of the baseline level were more common among patients in the hydrochlorothiazide groups than among those in the placebo group.
Conclusions
For patients with recurrent calcium oxalate stones and higher than desired urinary calcium, thiazide diuretics can be considered preferably in higher doses to lower urinary excretion provided adverse effects are monitored.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Bhavin Mandowara is a practising nephrologist at Zydus Hospital, Ahmedabad.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
