How to manage scorpion sting patients: Dr. H Bawaskar explains
M3 India Newsdesk Sep 27, 2018
Dr. H Bawaskar, well-known for his work and research on scorpion stings, details on the management of scorpion sting patients.

Haemodynamic
Karnad DR from India studied the haemodynamic pattern in 8 scorpion sting cases of Mesobuthus tamulus stings. He recorded severe vasoconstriction and hypertension in mild envenoming, while predominant left ventricular dysfunction with normal systemic vascular resistance causing pulmonary oedema or severe hypotension was related to fluid balance.
Warm shock with or without pulmonary oedema is the result of biventricular dysfunction and irreversible vasodilatation. Increased systemic pressure without rise in systemic vascular resistance is attributed to rise in cardiac output, an inotropic phase, where vasodilators are preferred.
- Inotropic phase is an early phase of envenomation characterized by hypertension and enhanced ventricular contractility.
- Hypokinetic phase the hallmarks of which are, hypotension and shock, reflect the alter left ventricular contractility. Dobutamine is preferred.
- Electron microscopes study of fatal scorpion sting victim showed contraction band necrosis with ruptured and hypercontraction sarcomeres as a result of excessive catecholamine similar to pheochromocytoma.
Echocardiographic changes
- Echo shows poor global myocardial contractility within 12 to 15 hours of sting, with low ejection fraction, decreased left ventricular performance, trivial mitral regurgitation, abnormal diastolic filling for five days to four weeks.
- Diminished or hypokinetic left ventricular global movement with decreased systolic function can be seen in scintigraphic study.
- At times systolic and frames show no change in diameter; flat septum with no systolic thickening. At times, the ballooning of the apex of the heart is attributed to stress-induced cardiomyopathy (Takotsubo). There is a good correlation between clinical improvement and the return of the left ventricular wall motion toward normal due to Mesobuthus tamulus sting.
- Serial echocardiography is useful to follow changes in left ventricular function and check the possibility of development of cardiomyopathy.
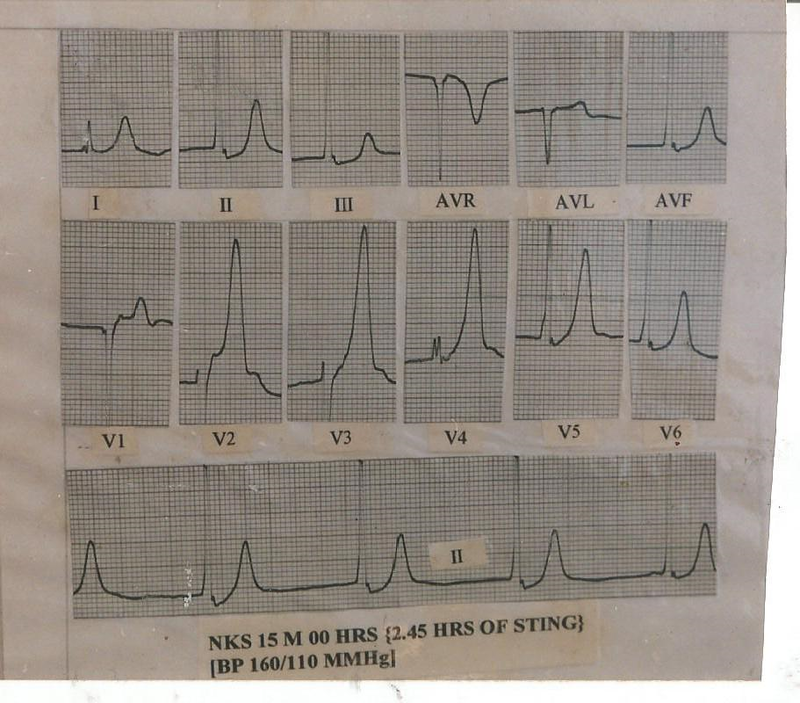
Electrocardiogram
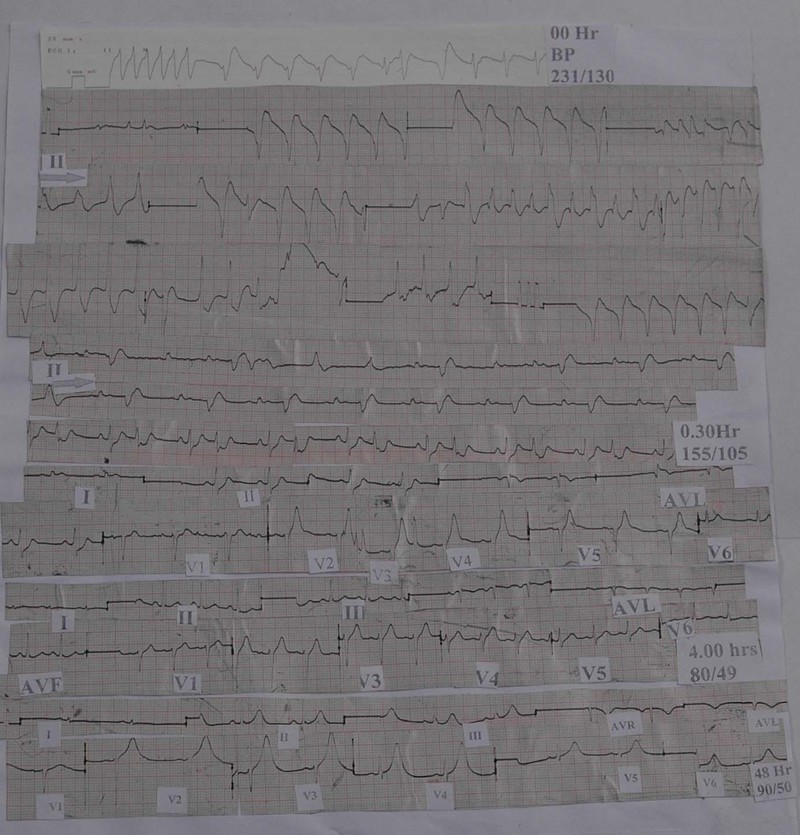
Dynamic ECG changes seen in scorpion sting victim with transient ventricular tachycardia, fascicular tachycardia, atrial fibrillation , AV dissociation and tented T waves
Tented T waves
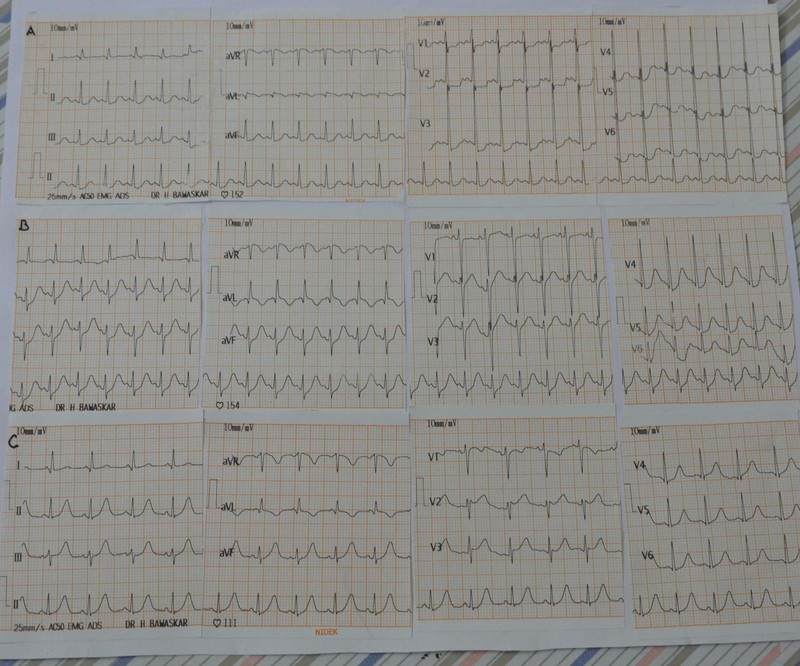
Tachycardia with subsequent recovery in a 6 years child treated with ASV, dobutamine, oxygen and BiPap
- ECG is the most important and easily available diagnostic tool in rural settings. No victim with systemic involvement shows normal ECG. RST segment and T waves are most frequently affected. Arrowhead tented T wave looks like the Ashoka tree and indicates acute injury, while tent-shaped T waves look like a Christmas’s tree and indicate recovery.
- Early myocardial infarction-like pattern, atrial arrhythmias, non-sustained ventricular tachycardia and various conduction defects due to injury to the conducting system can occur. PQRST or T waves alternans suggest serious myocardial injury.
- Prolonged QTc and conduction defect restore to normal within one week, T wave inversion persists for a few weeks. Low voltage, wide QRS complex, tachycardia, hemiblock, and mark ST segment depression carries a bad prognosis. At times, despite good clinical status, a victim ECGs showed mark abnormality.
Chest X-ray
Cardiogenic pulmonary oedema is characterised by unilateral distribution or batwing appearance of lung oedema due to left ventricular failure, due to simultaneous localised increase in pulmonary vascular permeability induced by venom.
While the patchy and peripheral distribution of lung oedema with air bronchograms are the radiological feature of pulmonary oedema due to increased vascular permeability.
Laboratory investigations
Raised leukocyte count in the range of 11400-41400 per/cu/mm within an hour of the sting can be seen. Rise in cardiac enzyme, cytokines, platelet activating factors, rennin, angiotensin II, serum potassium, urine and serum catecholamine, hyperglycemia, serum amylase, NT-proBNP level, and reduction in insulin level occurs in a victim of severe scorpion envenomation with severe cardiovascular damage.
Management
In the past, irrespective of various regimens including decongestive agents, lytic cocktail, propranolol and insulin-glucose drip, the fatality due to scorpion sting was between 20 to 29%. Since the advent of scorpion antivenom, vasodilators, and intensive care facilities the fatality is almost negligible in severe envenoming. Fluid loss due to vomiting, sweating and salivation may complicate the clinical course. Every effort should be made to correct the fluid balance.
Scorpion Antivenom
- Scorpion antivenom (SAV) must be administered as early as possible and through intravenous route. Mesobuthus tamulus envenoming causes transient parasympathetic and prolonged sympathetic stimulation.
- Signs and symptoms suggestive of parasympathetic stimulation indicate circulating unbound venom and can be neutralized by antivenom. Thus, by neutralizing circulating venom, SAV subsequently prevents the sympathetic overstimulation and its consequences.
- SAV is a specific treatment of scorpion sting therapy that has been a matter of debate and controversy during the last five years. But, recent randomized controlled trials have overcome the controversy regarding beneficial effects of early administration of SAV. Since 2002, nonspecific F(ab)2 SAV has been available for clinical use from Haffkine Biopharma Mumbai.
- Mesobuthus tamulus is common in western Maharashtra, Saurashtra, Kerala, Andhra Pradesh, Tamil Nadu and Karnataka where morbidity and mortality due to stinging have been reported.
Prazosin
Prazosin is widely used for the management of Mesobuthus tamulus sting. Bawaskar and Bawaskar did a prospective, randomized trial of scorpion antivenom plus prazosin versus prazosin alone in the treatment of severe Mesobuthus Tamulus sting at a general hospital Mahad, authors randomized 70 cases (antivenin plus prazosin 35) and (prazosin alone 35).
| Clinical Sign | Prazosin | Prazosin + Antivenom | P |
| Sweating, mean (SD) hours | 6.6 (2.60) | 3 (1.1) | 0.001 |
| Salivation, mean (SD) hours | 3 (1.9) | 1.9 (0.9) | 0.008 |
| Priapism, mean (SD) hours | 9.4 (1.5) | 4.7 (1.5) | 0.001 |
| Cold extremities, mean (SD) hours | 17.3 (6.6) | 8.5 (5.3) | 0.001 |
| Number with hypotension | 19 (54.3) | 12934.30 | 0.001 |
Bawaksar HS and Bawaskar PH- BMJ 2010;341:c7136 doi /10;1136/bmjc/136
- Patients in the antivenom plus prazosin group required significantly (p <0.001) fewer doses of prazosin than the prazosin group.
- The study concluded that the addition of scorpion antivenom to prazosin enhances recovery time and shortens hospital stay in patients with grade 2 Mesobuthus tamulus envenomation. The maximum volume of venom injected in one sting by an Indian red scorpion is 1.5 mg, and each ml of antivenom is capable of neutralizing 1.2 to 1.5 mg venom.
- Hence, we used 30 ml of antivenom. However, more may be required for severe sting. No participant had a mild or severe reaction to antivenom. High circulating catecholamine-induced by venom prevents reaction to antivenom and acts as prophylaxis against anaphylaxis.
- Vasodilators hydralazine, isosorbide dinitrate, nifedipine have been advocated for the treatment of scorpion sting.
- These agents cause reflex tachycardia and increase myocardial oxygen demand.
- Massive life-threatening pulmonary oedema where time is a great enemy necessitates rapid unloading and vasodilatation by sodium nitroprusside drip or nitroglycerine.
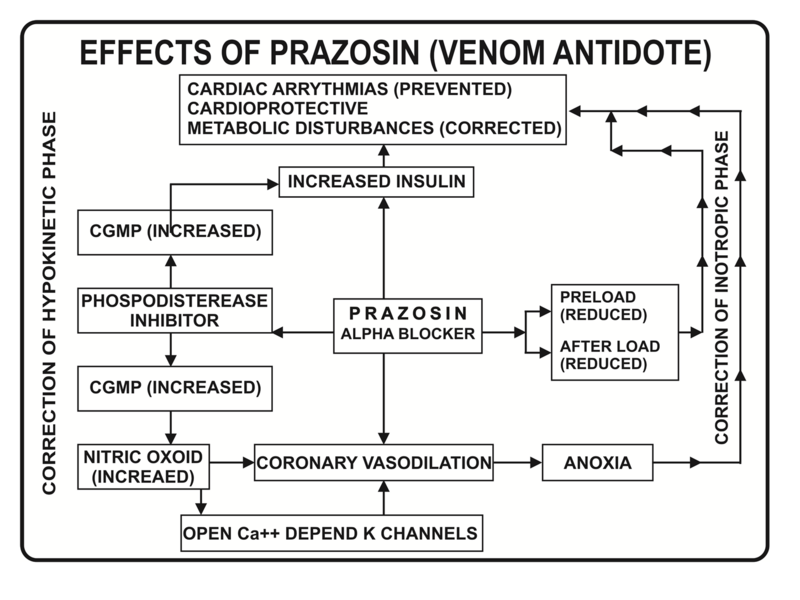
Alpha receptors stimulation plays an important role in the pathogenesis of scorpion sting. Prazosin is a phosphodiesterase inhibitor. It reduces preload and left ventricular impedance without raising heart rate. Prazosin is a simple scientific pharmacological and physiological antidote to scorpion venom actions, and it is easily available in rural setting.
In an experimental study support that scorpion sting involvement of peripheral alpha-1 adrenergic receptors for pressure response this is the reason why prazosin an alpha-1 blocker has been successfully used to reverse ill effects of circulating catecholamines.
Impressive reduction in case fatality from Mesobuthus tamulus sting 26% in 1961 and 6% in 1980 and currently <1% shows that it is possible when dedicated care is available at specific centres. In endemic regions, the prazosin is a darling amongst drugs kept ready on the outpatient department tray. Even, two tablets are carried in the purse by consultants of these areas.
- Victims presented with hypokinetic phase due to both ventricular dysfunctions clinically characterized by hypotension, shock, tachycardia, delirium, with or without pulmonary oedema and warm extremities, and improved with dobutamine infusion of 5 to 20 microgram/kg/mi.
- 7 out of 11 children had myocardial dysfunction and decompensate shock in addition to dobutamine responded to nitroglycerine (NTG) drip 0.5 to 5 microgram/pe/min by improving heart dysfunction and reduction in pulmonary congestion.
Venodilator action of nitroglycerine (NTG) reduces the preload of the heart and it improves the intrapulmonary shunting and also relaxes the pericardial coronary arteries and its collaterals. Pulmonary oedema cases improve with dobutamine, mechanical, or non-invasive ventilation or by helmet-derived non-invasive pressure support ventilation.
Final protocol- Management of scorpion sting
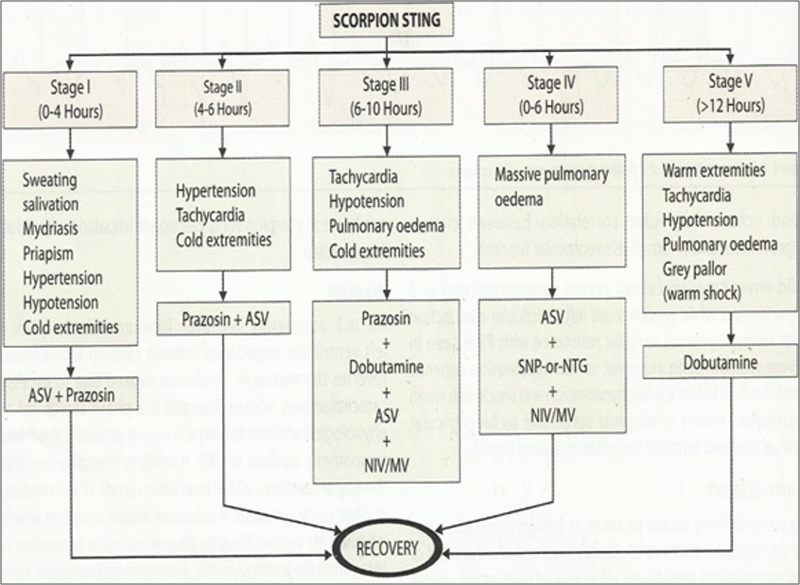
ASV- Scorpion antivenom, NIV (Non-invasive ventilator), SNP-sodium nitroprusside, NTG-nitroglycerine, MIV- Mechanical ventilation
Prevention
False ceiling under loose tiles of roof and use of bamboo cot with scrupulous use of mosquito net can protect from a scorpion sting. In endemic areas, clothing, bedding, shoes, and packages should be vigorously shaken out and checked for scorpions without blindly using it. Sandals do not prevent stings. Pesticides like organophosphates, pyrethrins, and chlorinated hydrocarbons are known to kill scorpions. One should not sit touching mud walls. At times of opening the school, the tables and rooms (roof, walls and floor) should be thoroughly cleaned and washed.
Conclusion
Early hospitalization and administration of an accurate dose of scorpion antivenom, prazosin, and closely monitoring the victim in intensive care unit will save many laminated lives. Periodic training for peripheral doctors regarding management of scorpion sting should be arranged. Scorpion sting should be included as a notifiable disease and in regular medical teaching at least in tropical and subtropical countries.
Click to read Part 1 of the series- How to identify scorpion sting: Dr. H. Bawaskar explains
The writer, Dr. Himmatrao Bawaskar is a renowned Indian physician with publications in The Lancet. He has done extensive research in scorpion sting- diagnosis and treatment protocol.
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author did not accept any payment for the article.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
