Erectile dysfunction: What is the current treatment?
M3 India Newsdesk Jul 24, 2022
Erectile dysfunction (ED) is the most common sexual problem in men that causes a substantial negative impact on intimate relationships, quality of life, and self-esteem. This article highlights the major treatment protocols for ED that can be used by physicians.
Erectile dysfunction
The incidence increases with age and affects up to one-third of men throughout their lives. Male sexuality, a complex physiological process, is an important part of the quality of life.
The maintenance of normal sexual function depends on the coordination of the human multi-system, involving the coordination of the nervous system, the cardiovascular system, the endocrine system and the reproductive system. When these systems or psychosocial aspects are changed, it will affect the quality of normal sex life for any individual.
In men, sexual function declines over time, beginning during the fifth decade and affecting all domains of sexual health including desire, arousal, erectile function, and ejaculation/orgasm.
Erectile dysfunction (ED) also negatively affects a man's relationships, emotional and psychological well-being, and partner relationships. It causes a substantial negative impact on intimate relationships, quality of life, and self-esteem.
Risk factors for ED
Erectile dysfunction is the persistent inability to achieve or maintain a penile erection satisfactorily for sexual performance and is the most common male sexual disorder, with 44% of men 60-69 years old and up to 70% of men ≥70 years old endorsing erectile difficulties; in men <40 years old, ~5 % endorse ED.
There are two major subtypes of ED:
- Lifelong ED: in which erection cannot be achieved from the outset of sexual desire
- Acquired ED: in which ED begins after a period of normal erectile and sexual activity
Each of these subtypes can have either psychogenic or organic contributors.

Treatment of erectile dysfunction
The treatment of ED comprises psychosexual therapy, lifestyle modifications, and medical and surgical interventions. Psychotherapy is considered as a first-line ED therapy, is both noninvasive and effective, and can be combined with other therapies.
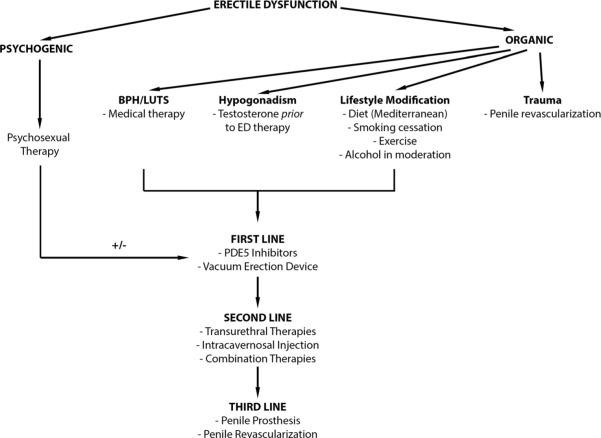
Lifestyle modification in men with ED
It is believed that lifestyle adjustments in men with ED not only reduce cardiovascular risk but also improve ED symptoms. Lifestyle alterations such as smoking cessation reduce cardiovascular mortality by 36%, physical activity results in 30-50% reductions in Diabetes mellitus and Coronary artery disease incidence, and diet reduces death from CAD by up to 36%.
Based on these findings, recommended lifestyle alterations include regular exercise, smoking cessation, dietary intervention with emphasis on the Mediterranean like diet, as well as moderate alcohol consumption.
Hypogonadism and ED
Testosterone supplementation is often recommended in hypogonadal men with ED, which may ameliorate both ED symptoms as well as cardiovascular risk.
Studies have shown a 57% overall response rate to testosterone monotherapy in men with ED, with an improvement in erectile function in 39% of men, as well as improvements in sexual performance, desire, and motivation. Testosterone supplementation should begin prior to treatment with ED-specific medications.
Oral therapies
Phosphodiesterase 5 inhibitors are first-line medical therapy for ED and encompass numerous drugs including the first-generation drugs:
- Sildenafil (Viagra®)
- Vardenafil (Levitra®)
- Tadalafil (Cialis®)
Sildenafil, tadalafil, and vardenafil are the most popular ED drugs in current use. Sildenafil was the first PDE5i approved for ED treatment, has a time of onset of 30 min and an 8-h duration of clinical efficacy. Both sildenafil and vardenafil have a delayed onset of action after fatty food ingestion.
In contrast, tadalafil has a longer time of onset of 2 hours, with a 36-hour duration of efficacy and with no interaction with food.
Transurethral therapies
While limited in its utility, transurethral alprostadil (prostaglandin E1 (PGE1)) is a reasonable first-line or combination ED therapy. First brought to market in 1994 and marketed as Medicated Urethral System for Erection (MUSE®), transurethral alprostadil has shown limited efficacy, with response rates of 27 to 53%.
However, combination therapy with sildenafil has been shown to salvage the effects of MUSE®. The system is also beneficial in men whose penile nerves have been compromised as it bypasses the need for intact neurological pathways for erection.
Intracavernosal therapies
Intracavernosal injection therapies constitute a second-line ED treatment and are often used when oral therapies fail. Like MUSE®, injectable therapies bypass the need for intact neurological pathways for erection. These include various combinations of PGE1, phentolamine, papaverine, and vasoactive intestinal peptide (VIP).
When used alone, PGE1 results in high rates of erections usable for sexual intercourse. A combination of papaverine and phentolamine, marketed as Androskat® but commonly referred to as Bimix, is also available. Bimix has an efficacy rate of 94 % with a side effect incidence of 0.9–2.6% for prolonged erection, pain, or hematoma.
Surgical therapy in men with ED
The spectrum of ED treatment is incomplete without mention of some invasive therapies such as penile prostheses and penile revascularisation procedures.
Penile prosthesis
Insertion of a penile prosthesis is considered as the third-line therapy for ED, used after patients fail medical therapies. Penile prostheses are available in semirigid and inflatable forms, with the inflatable form being the most popular.
The semirigid prosthesis is easier to implant and maybe a better option for men with poor manual dexterity and difficulty using the pump of the inflatable prosthesis. Penile prostheses require replacement every 8 to 15 years, and the most common complication after implantation is infection.
Penile revascularisation surgery
Approaches to penile revascularisation include repair of arterial stenosis and penile venous ligation, depending on the ED aetiology. This therapy can be offered to nonsmoking, nondiabetic men who are <55 years old with isolated arterial stenoses without generalised vascular disease.
The principles guiding penile revascularisation include anastomosis of the inferior epigastric artery to the dorsal penile arteries and/or the deep dorsal vein.
Conclusion
Erectile dysfunction significantly limits the quality of life of a growing number of men. Given the rise in the number of predisposing factors due to sedentary lifestyle and dietary choices, ED has been affecting a larger population in every upcoming year. The spectrum of treatment ranges from minor lifestyle changes to major surgical interventions.
Continued research into the molecular mechanisms of ED and the development of improved medications will further expand the significant armamentarium of treatments currently available, improving not only the quality of life of affected men but also their life span.
This article was originally published on 11 November 2021.
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
