Cerebral Palsy: Oral Manifestations & Dental Management
M3 India Newsdesk Jan 15, 2025
The aetiology, classification and oral manifestations of cerebral palsy are elucidated in this article. This article also mentions the levels of the Gross Motor Function Classification System GMFCS 2008.
The American Academy for Cerebral Palsy and Developmental Medicine describes cerebral palsy as a group of disorders of movement and posture development, causing activity limitations that are attributed to nonprogressive disturbances in the developing foetal or infant brain.
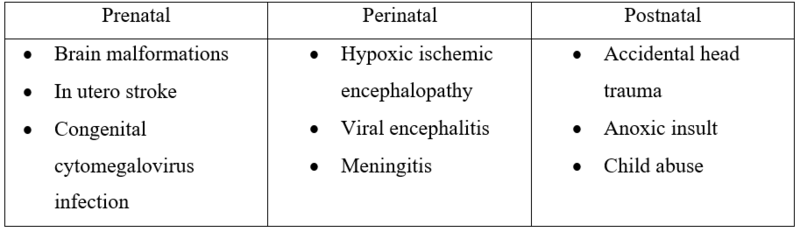
Aetiology
4 P’s: prenatal, perinatal, postnatal, and prematurity, out of which the first 3 are more common.
Classification
- Spasticity
- Athetosis (dyskinetic)
- Ataxia
- Mixed
1. Spasticity
- It comprises 50–70% of cerebral palsy patients.
- It is characterised by increased muscle tension.
- Excessive involuntary contractions when the muscle is stretched.
- Limited control of neck muscles leading to neck roll.
- Lack of coordination of oral and perioral muscles leads to impaired chewing, swallowing, tongue thrusts and speech impairments.
2. Dyskinetic
- Characterised by purposeless involuntary muscular contractions.
- It comprises 15% of all cerebral palsy patients.
- Athetosis is a succession of slow, twisting or writhing involuntary movements.
- Choreoathetosis—quick jerky movements.
- Frequent uncontrolled jaw movements cause abrupt closure of the jaws or severe bruxism.
- Hypotonicity of oral and perioral muscles leads to drooling, speech disturbances, impaired swallowing, chewing and tongue thrusting.
- Facial grimacing.
3. Ataxic
- It comprises 5% of cerebral palsy patients.
- Loss of muscular coordination leads to imbalance and an unsteady gait.
- Difficulty in grasping objects.
4. Mixed
- It comprises approximately 10% of all cerebral palsy patients.
- Features comprising a combination of characteristics of all three types of cerebral palsy.
Gross Motor Function Classification System GMFCS (2008)
- Level I – Walks without limitations
- Level II – Walks with limitations
- Level III – Walks using a handheld mobility device
- Level IV – Self‑mobility with limitations may use powered mobility
- Level V – Transported in a manual wheelchair.
Oral manifestations
- The prevalence rate of malocclusion has been reported between 59 and 92%, with the vast majority of malocclusion classified as Angles Class II with increased over-jet and overbite, unilateral cross-bite and open bite associated with abnormal oral habits is twice more common.
- This is because of the following reasons:
- Uncoordinated movement of jaws lips and tongue.
- Mouth open posture with postural tongue thrust and mouth breathing.
- The prevalence of dental trauma was 36.3%; enamel fracture was the most common trauma (89.1%).
- There was the highest prevalence of TDI in cerebral palsy patients with hemiplegia (40.6%).
- A high prevalence of bruxism in individuals who have Cerebral Palsy has been reported in many studies.
- The prevalence of periodontal disease is higher. This is because of the following reasons:
- Poor manual dexterity of the child to perform good oral hygiene measures
- Anti–convulsant medication induced gingival enlargement
- The incidence of caries among children and adolescents who have Cerebral Palsy is high but another study concluded that in both dentitions, individuals with cerebral palsy have less chance of having caries than the subjects in the comparison groups.
- Dental erosion is common in Cerebral Palsy patients, and dentists should be alert towards early signs of erosion in cerebral palsy patients and provide appropriate preventive therapy. It was concluded that erosive tooth wear (ETW) in Cerebral Palsy children is associated with frequent consumption of soft drinks, and powdered juices, and reported gastro-oesophageal reflux.
- Most of the affected teeth observed in the Cerebral Palsy group were upper molars (54%), lower molars (58%) and upper incisors (54%).
- The sequence of eruption in children with CP was almost similar to the normal. Except the second premolar and the second molar which shows delayed eruption.
- It was found that a high prevalence of developmental enamel defects was found among children with CP.
Treatment
The treatment consideration involves four points, which are as follows:
1. Intellectual maturity and cooperative ability:
- The intellectual maturity and the proportional cooperative ability are assessed.
- Based on this assessment, children are classified as educable, trainable and nontrainable.
2. Postural compliance in the dental chair:
- The manifestation of enhanced muscular rigidity, hypercontractility, Jerky and/or uncoordinated movements, and staggering or ataxic gait may compromise the compliance of the child to lie down on a dental chair.
- If the child is not able to get onto the dental chair, an examination may be rendered on a chair where the child can be comfortably seated.
- If the child is wheelchair-bound, dental examination/incited treatment may be carried out as the child is seated in the wheelchair.
3. Systemic complications:
The presence of systemic complications necessitates an assessment by the plan. The physician's opinion about the fitness of the child to undergo a particular procedure is required.
4. Preventive care:
Preventive care comprising good oral hygiene practices, training and awareness of oral hygiene practices to the caretaker, fluoride application, sealant application and periodic reviews are emphasised.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Neha Kalantri is a practising dentist from Nashik.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
