Which calcium channel blockers should be used in hypertension; Amlodipine, Cilnidipine, or Benidipine?
M3 India Newsdesk Feb 27, 2019
Prof. Dr. Sundeep Mishra expertly takes you through the maze of calcium channel blockers and talks about newer agents that could possibly replace the older ones.
Hypertension affects more than 1 billion individuals worldwide. Hypertension is the single-most common reason to visit a doctor and is a major risk for cerebrovascular diseases (cardiac disease and stroke) and the second-leading cause of end-stage CKD. So many diseases can be attributed to it that it becomes the single most important cause of mortality worldwide. Thus while the burden of hypertension is enormous the good part is that it is an eminently manageable chronic condition.
Several studies have demonstrated that a 5–6 mmHg decrease in diastolic blood pressure can reduce the risk of stroke, coronary heart disease and even mortality. Clinical trial experience has demonstrated that treatment of hypertension reduces CVS disease outcomes, including incident stroke (35 - 40%), MI (15-25%), and heart failure (up to 50%).
Unfortunately the control of hypertension has neither been able to meet the goals as determined by guidelines or public health administrators (65% in Million Hearts Initiative by 2017) even in West what to speak of low resource countries.
Several classes of antihypertensive agents can achieve effective control of blood pressure; diuretics, α-blockers, β-blockers, angiotensin converting enzyme (ACE) inhibitors, angiotensin II type 1 receptor blockers (ARB), and organic calcium channel blockers (CCBs). Among them, β-blockers have significant side-effects and α-blockers are known to increase mortality and therefore are no longer preferred as primary therapy in uncomplicated hypertension but others diuretics, ACE-Inhibitors, ARBs and CCBs are considered first-line therapy. Among them, CCBs are not only potent but also decrease morbidity and mortality associated with hypertension. Based on the chemical structure, CCBs are categorised into 3 subgroups;
- Phenylalkylamines: verapamil and gallopamil
- Benzothiazepines: diltiazem and clenazem
- Dihydropyridines: nifedipine, nicardipine, felodipine, amlodipine, benidipine aranidipine, azelnidipine, cilnidipine, efonidipine, manidipine and nilvadipine
Phenylalkylamines have predominantly negative into and/or chronotropic effect and therefore used as anti-arrhythmic but are not very useful as an anti-hypertensive agent.
Benzothiazepines also similar albeit a bit weaker action and therefore is also not very useful in this context.
Dihydropyridines, on the other hand, exert a vaso-dilator action on vascular smooth muscle cells by inhibiting calcium entry through L-type calcium channels with minimal/no action on iono/chronotropicity rather they cause reflex tachycardia due to peripheral vasodilation and thus find much use in hypertension.
Recently, newer types of CCBs have been developed which may manifest N-channel blocking activity (cilnidipine) and/or T- (benidipine, mibefradil and efonidipine) type calcium channel blocking activity along with the usual L-type channels.
These additional channel blocking activities can lead to additional benefits with further reductions in cardiovascular events and renal injury. However, the only question is whether these effects are beneficial in the clinical setting.
Dihydropyridines CCBs available in clinical practice
Earliest available CCBs, nifedipine, nicardipine, verapamil, and diltiazem were short acting. Several reports with short-acting CCBs reported increased mortality.
This led to the development of CCBs with a longer duration action and pharmacokinetic profile with enhanced L- type of vascular selectivity like nifedipine SR (slow release), felodipine ER (extended release), diltiazem SR and amlodipine.
Later on, other types of calcium channels were also discovered like N- type (Cilnidipine) and drugs with action on all 3 channels; L, N and Type (Benidipine). Since N-type channel is found distributed along the nerve and in the brain, cilnidipine is anticipated to exert a specific action on nerve activity, such as inhibition of the sympathetic nervous system.
T-type of channel is distributed in kidney therefore benidipine is likely to have reno-protective effects as well, in addition to the action on the sympathetic nervous system and blood vessels.
CCBs and Hypertension
Several trials demonstrated that short-acting CCBs like Nifedipine could increase heart rate and increase angina, worsened angina but even more importantly mortality in a dose-dependent manner.
Likewise, diltiazem another short-acting agent exerted no overall effect on mortality or incidence of reinfarction in postinfarction patients.
ASCOT-BPLA study revealed that the amlodipine-based regimen could reduce the incidence of CV diseases and inhibit the progress of diabetes compared with that of atenolol-based regimen.
Likewise, in the JMIC-B trial, nifedipine-retard preparation has been found as effective as ACE - Inhibitors in preventing cardiac events and mortality in patients with hypertension and CAD.
Newer generation CCB, cilnidipine was found to suppress cardiac sympathetic overactivity in patients with essential hypertension contributing to a decrease in mean blood pressure, with relatively less effect on heart rate, rather decreasing the incidence of ventricular premature beats. Clinically, it was also found to reduce the white coat effect in patients with essential hypertension.
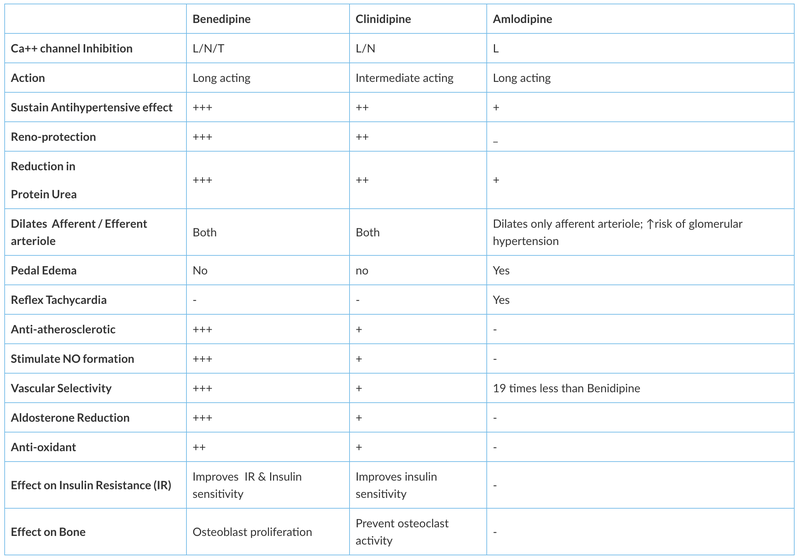
Benidipine hydrochloride is another new CCB found to inhibit the T-type as well as L- and N-type calcium channels. Benidipine, via blockade of T-type calcium channels, seems to exert a more protective effect against cardiorenal injury vis a vis cilnidipine, through more attenuation of oxidative stress and the reduction of aldosterone. Comparisons of commonly available CCBs are given in the figure.
Several studies have demonstrated that benidipine favourably affect renal function in patients with essential hypertension compared with amlodipine, suggesting that the clinical benefits of benidipine as an antihypertensive drug.
Likewise in another study, benidipine was found to possess a more potent antihypertensive effect than cilnidipine as well as a renoprotective effect, indicating the high usefulness of benidipine in hypertensive patients with diabetes.
Thus T-type calcium channel blockade is most possibly involved in the renoprotective effect of benidipine.
Figure: Comparison of Amlodipine, Cilnidipine, and Benidipine
Conclusion
Newer CCBs like benidipine and cilnidipine are poised to replace older agents like amlodipine. These newer agents are not only effective anti-hypertensive agents but have an additive sympathetic blockade and reno-protective effects as well.
Disclaimer-The information and views set out in this article are those of the author(s) and do not necessarily reflect the official opinion of M3 India. Neither M3 India nor any person acting on their behalf may be held responsible for the use which may be made of the information contained therein.
The writer, Dr. Sundeep Mishra is a Professor of Cardiology.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
