'How can the immune system be restored to fight cancer cells?': Dr. Anurag Mehta & Dr. Garima Gupta
M3 India Newsdesk Feb 01, 2019
The continuous monitoring and removal of transformed cells is called immunosurveillance, but subversion can allow cancer cells to escape and grow. Slippages occur that lead to the transformed cells escaping elimination and establishing a full-blown tumour. During such an event how can the immune system be restored to fight?
Cancer immunity cycle while protective against cancer has inherent checks and balances primarily from their role in infection control where the immune process must abate once the infection has been removed. The system works efficiently even in recognising and eliminating the transformed cells on daily basis. However, slippages occur that lead to the transformed cells escaping elimination and establishing a full-blown tumour.
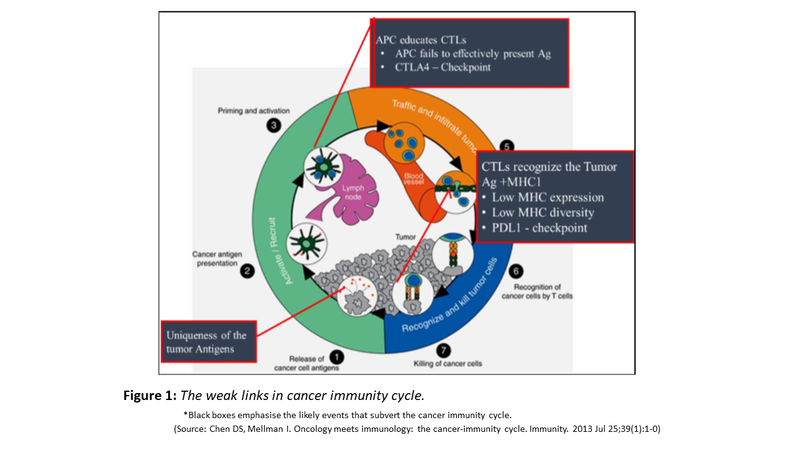
While scrutinising the cancer immunity cycle, one can identify several vulnerable spots that can hamper the efficacy of immunosurveillance. These vulnerable events are shown in black boxes in Fig. 1. To enumerate those:
- Tumour does not produce unique/immunogenic Ags. Tumours with a low level of mutations such as those driven by a single driver mutation like biomarker positive Non-Small Cell Lung Cancer (NSCLC), Adenoid Cystic Carcinoma, Mucoepidermoid carcinoma and many others fail to produce potent neoantigens. In contrast, tumours with DNA damage response insufficiencies especially those with pathogenic mutations in DNA Polymerase Delta 5’-3’ exonuclease domain and Mismatch Repair Pathway produce highly mutated tumours with a great possibility of producing immunogenic neoantigens.
- Tumour cells downregulate MHC1 expression or lose MHC genes as a part of genetic instability. Since all class 1 MHC molecules reside in chromosome 6p and are tightly packed together, loss of 6p can result in loss of one haplotype of HLA class I. Reduced diversity of MHC class I molecule weaken the effectiveness of APCs in exporting MHC restricted tumour antigens.
- Crucial genes involved in the immune response have been lost and an immune desert phenotype is produced.
- Recruitment of immunosuppressive cells to the tumour microenvironment happens, especially due to checkpoint inhibition that transforms CTLs to Tregs with immunosuppressive activity. In addition, Tumour-Associated Macrophages (TAM) and Myeloid Derived Suppressive Cells (MDSC) enrich in the tumour microenvironment. What invites TAM & MDSC is not clear as yet but these seem to be significant contributors to tumour growth despite a tumour inflamed phenotype.
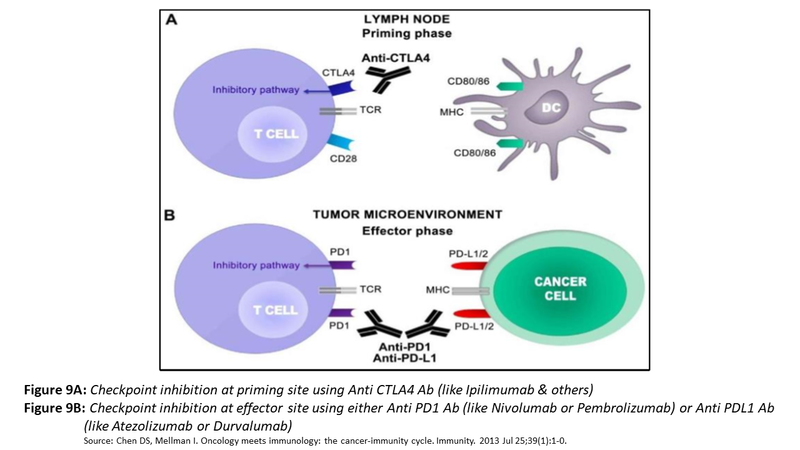
- Resistance to cytotoxicity: Checkpoint activation at priming site and effector site halt the progression of immune destruction of cancer cells and additionally, lead to depletion and anergy of CTLs. Not only that, checkpoint inhibition also propels conversion to CTLs to Tregs.
How can the immune system be restored to fight cancer cells?
The objective of cancer immunotherapy is to restore the cancer immunity cycle by buttressing the weak spots in a manner that replicates the normal but does not go overboard to generate unrestrained autoimmune responses. The various strategies that have been used with different levels of success are depicted in Fig. 2 below.
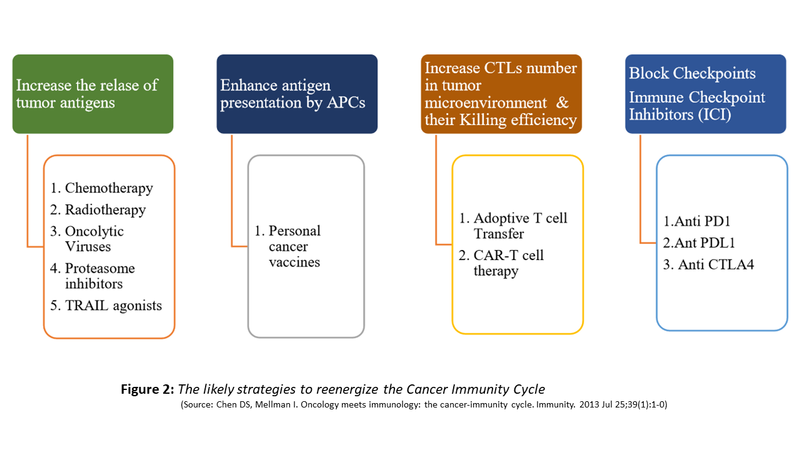
Of these, three strategies have received FDA approval.
- Personal cancer vaccine Sipuleucel-T which is a Dendritic Cell Vaccine for treatment of asymptomatic Androgen-Independent Prostate Cancer (AIPC) was first given accelerated approval in 2005.
- Chimeric antigen receptor (CAR) T-cell therapy is a type of immunotherapy that uses a patient’s own genetically modified T cells to find and kill cancer.
- KYMRIAH and YESCARTA are two FDA approved bioengineered patient’s T cell that has been multiplied in the lab and has a recognition site for CD19 molecule.
These have FDA approval for a variety of B cell Malignancies. But the greatest advance has been development and widespread usage of Immune Checkpoint inhibitors (ICIs). Five of these have been accorded FDA approval. These work by imposing an antibody barrier between receptor and ligand causing restraint on the checkpoint and freeing the CTLs to carry out their task of identifying tumour cells and neutralising them.
Several Studies have shown durable clinical benefit in up to 40% of selected patients with advanced cancer. The various trials till May 2018 with results are shown in the table below.
| Drug Class | Target | Agent | Diseases with trial results reported |
| CTLA-4 inhibitors | CTLA-4 |
Ipilimumab (Yervoy) |
Melanoma Non-Small Cell Lung Cancer Small Cell Lung Cancer Renal Cell Carcinoma |
| Tremelimumab | Melanoma | ||
| PD-1 inhibitors | PD-1 |
Nivolumab (Opdivo)
|
Hodgkin's Lymphoma Melanoma Non-Small Cell Lung Cancer Small Cell Lung Cancer Hepatocellular Carcinoma Renal Cell Carcinoma Ovarian Cancer Head and Neck Cancer Urothelial Cancer Colorectal Cancer (MSI-H/dMMR) |
| Pembrolizumab (Keytruda) |
Melanoma Non-Small Cell Lung Cancer Small Cell Lung Cancer Head and Neck Cancer Urothelial Cancer Triple Negative Breast Cancer Mesothelioma Hodgkin's Lymphoma Gastric Cancer Solid Tumours (MSI-H/dMMR) Colorectal Cancer (MSI-H/dMMR) |
||
| PD-L1 Inhibitors | PD-L1 | Durvalumab (Imfinzi) |
Urothelial Cancer Head and Neck Cancer Non-Small Cell Lung Cancer |
| Atezolizumab (Tecentriq) |
Urothelial Cancer Melanoma Non-Small Cell Lung Cancer Renal Cell Carcinoma Triple Negative Breast Cancer |
||
| Avelumab (Bavencio) |
Merkel Cell Carcinoma Urothelial Cancer |
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
Dr. Anurag Mehta, a senior pathologist with more than 30 years of experience in the field, and special interest in molecular biology and diagnostics is also the Director - Department of Laboratory & Transfusion Services and Director Research, Rajiv Gandhi Cancer Institute, N Delhi.
Dr. Garima Gupta is a Senior Research Officer at Rajiv Gandhi Cancer Institute, N Delhi.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
