Simplified in Practice: ECG basics & how to interpret
M3 India Newsdesk Jun 17, 2021
Many general clinics include an ECG machine, which is a good screening test for cardiac issues. However, competent ECG analysis takes years to establish. This is not always straightforward for harried physicians. This article discusses many potential pitfalls for non-expert ECG interpretation. This is part one of our new series- Simplified in Practice.
ECG basics
When faced with an ECG, it is prudent, to begin with, the fundamentals: rate, rhythm, and axis. Then, with certain fundamental considerations in mind, consider the PQRST complexes in all the leads:
- Is the PR interval within the standard range (three to five small squares or 120 to 200 milliseconds)?
- Is it possible to have pathological Q waves?
- Is the QRS complex greater than 120 milliseconds in duration (>three small squares = bundle branch block [BBB])? The right BBB has a positive R wave in V1, whereas the left BBB exhibits a negative R wave in V1 and a positive R wave in lead V6.
- Do the R waves over the chest leads rise gradually and regularly (by V4, the R wave should be larger than the S wave)?
- Is there an anomalous ST dip or inversion of the T wave?
- Is the QT interval normal (a QTc value greater than 450ms may indicate ventricular tachycardia [VT])?
The ECG computer analysis should only be used as a guide.
Rate-recognising paper speeds
- The rate at which the ECG machine produces a trace is known as the paper output speed.
- The standard output speed is 25 mm per second.
- If a different paper speed is utilised, standard rate calculations will need to be adjusted accordingly.
- The standard paper speed is 25mm/sec:
- 1 mm (small square) = 0.04 sec (40 ms)
- 5 mm (large square) = 0.2 sec (200 ms)
ECG rhythm strip
250 SMALL squares = 50 LARGE squares = 10 seconds
To calculate beats per minute (bpm): 1500 SMALL squares = 300 LARGE squares = 1 minute
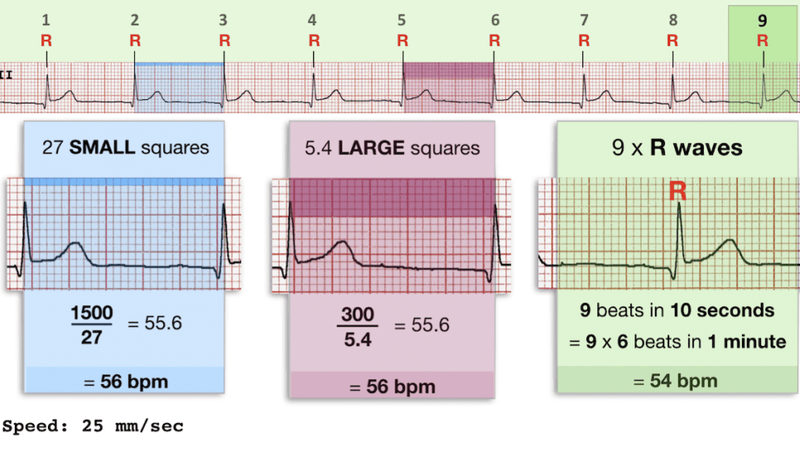
There are several techniques for calculating the rate:
The beats per minute (bpm) may be calculated by dividing 1500 by the number of SMALL squares between two R waves (one beat = R-R gap).
Divide 300 by the number of LARGE squares between two R waves (R-R interval Equals one beat) to get the beats per minute (bpm).
- Regular rhythms: Rate = 300 / number of LARGE squares between successive R waves.
- Very fast rhythms: Rate = 1500 / number of SMALL squares between successive R waves.
- Slow or irregular rhythms: Rate = Number of R waves X 6
The average rate during a ten-second period is given by the number of complexes (count R waves) on the rhythm strip. This is multiplied by 6 (10 seconds x 6 = 1 minute) to calculate the average beats per minute (bpm).
Rates of 60 to 100 bpm is considered normal. The rate is calculated by dividing 300 by the number of centimetre squares between complexes; a patient with two large squares between complexes has a heart rate of 150 beats per minute (a common rate for AF with 2:1 block), three large squares are 100 beats per minute, and six large squares is 50 beats per minute (a little on the slow side). Slow rates in athletes may be typical.
Rhythm
P waves in the sinus rhythm should be visible. Poorly controlled AF is the most frequent tachycardia; check for a fluctuating RR interval and the lack of crisp P waves.
ECG features of normal sinus rhythm:
- Regular rhythm at a rate of 60-100 bpm (or age-appropriate rate in children)
- Each QRS complex is preceded by a normal P wave
- Normal P wave axis: P waves upright in leads I and II, inverted in aVR
- The PR interval remains constant
- QRS complexes <100 ms wide (unless co-existent interventricular conduction delay present)
Sinus rhythm variations
- Sinus tachycardia = Sinus rhythm with resting heart rate > 100 bpm in adults, or above the normal range for age in children
- Sinus bradycardia = Sinus rhythm with resting heart rate < 60 bpm in adults, or below the normal range for age in children
- Sinus arrhythmia = Sinus rhythm with a beat-to-beat variation in the P-P interval (the time between successive P waves), producing an irregular ventricular rate
It might be difficult to perceive the abnormality when the pace is quick, but careful measurement will reveal it. AF is often asymptomatic and becomes more common as people get older. Supraventricular tachycardias (SVTs) and atrioventricular nodal re-entrant tachycardias are two other types of fast narrow complex tachycardias. These are frequently rapid, regular beats that are connected with palpitations in those who are younger.
Complete heart block (total lack of connection between P waves and QRS complexes), 2:1 block, and slow AF are all-important slow heart rhythms. Patients who have dizziness or blackouts are likely to require continuous pacing.
Axis
The axis is normal if leads I and II are both positive (this is from -30 to +90 degrees).
Normal Axis = QRS axis between -30° and +90°.
Abnormal axis deviation, indicating underlying pathology, is demonstrated by:
- Left axis deviation = QRS axis less than -30°
- Right axis deviation = QRS axis greater than +90°
- Extreme axis deviation = QRS axis between -90° and 180°
Examining LEAD I and LEAD aVF is the most efficient technique to estimate axis.
Determine if the QRS complex in each lead is positive, isoelectric (Equiphasic), or negative
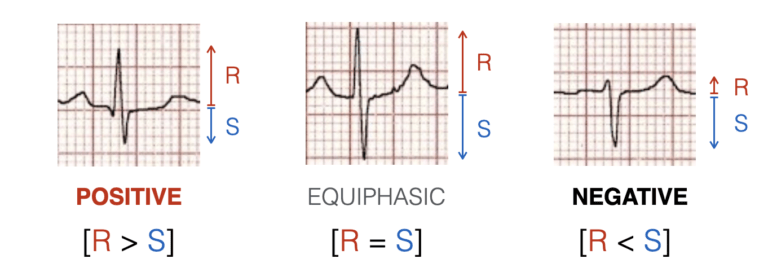
- If lead I is positive and II is negative, left axis deviation occurs. In the right axis deviation, I is negative and II is positive. Left ventricular hypertrophy (LVH) can cause left axis deviation as well as ST depression in the lateral leads. Right axis deviation occurs when the right heart is under stress, such as with pulmonary embolisms or an atrial septal defect.
- Isolated ventricular ectopic beats are rather frequent and seldom require therapy.
- Patients frequently report 'missing a beat' followed by a pounding heartbeat. They normally notice this when they're resting, and it's a good indication if it goes away while they're active.
- Broad complex runs are more ominous, especially if they are accompanied by blackouts or extreme dizziness. Although rhythms like rapid AF and SVT can generate BBB, it's safer to believe that all wide complicated runs (>3 beats) are caused by VT.
This is part one of our new series- Simplified in Practice where we break down ECG interpretation for various conditions. Stay tuned for more!
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author is a practising super specialist from New Delhi.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
