Chest CT: Can it aid in COVID-19 diagnosis in patients with first negative RT-PCR results?
M3 India Newsdesk Sep 24, 2020
Dr. Monish Raut elaborates on the role of HRCT as a valuable tool in confirming COVID-19 diagnosis and studying disease progression and severity among patients who test negative for RT-PCR initially. He also adds a note on the accuracy of the CO-RADS scoring system.
For our comprehensive coverage and latest updates on COVID-19 click here.
The RT-PCR test is said to be the gold standard to diagnose COVID-19. However there are possibilities that the initial phase of the disease may produce false-negative results which may be due to sub-optimal sampling or low viral load. Such patients, left undiagnosed and untreated, remain potential superspreaders in the community. Doing pre-operative testing has become the new normal, screening procedure before any elective procedure. A false negative patient undergoing surgery means a significant risk is exposed to not only healthcare workers but other hospitalised patients.
HRCT thorax evaluation confirmed disease findings in a significant number of patients with early false-negative RT-PCR result. Growing evidential studies have suggested HRCT chest as add-on primary tool for revealing COVID-19 disease during this pandemic time.
COVID commonly involves bilateral multifocal areas of the lungs. Single lobe involvement was also observed in a small number of patients. The right lower lobe, being a short and thick anatomic structure, can easily be invaded by the virus. Sub-pleural distribution of the disease is commonly seen because of possible location of target cells in the lower airway. Lesions around the bronchovascular pathways can be explained by the spread of infection along the intralobular interstitial tissues. Inflammation starts by early invasion of cortical pulmonary airways and alveolar epithelium, and gradual extension towards the central area.
Chest CT can be used to determine disease severity, progression, and staging of COVID-19 pneumonia. Pathological succession and CT features can be very well correlated.
| Early stage (days 0-4) | Ground-glass opacities |
| Progressive stage (days 5-8) |
Crazy paving patterns suggestive of recruitment of inflammatory cells to the lung interstitial space |
| Peak stage (days 10-13) | Consolidation due to tissue organisation and diffuse alveolar damage |
Apart from SARS-CoV-2, these radiological features can also be seen in other viral, atypical pneumonia and non-infectious inflammatory pulmonary conditions.
Typical findings:
- Ground-glass opacities with multifocal and peripheral or basal distributions
- Crazy paving
- Spider web
- Consolidation
- Reversed halo
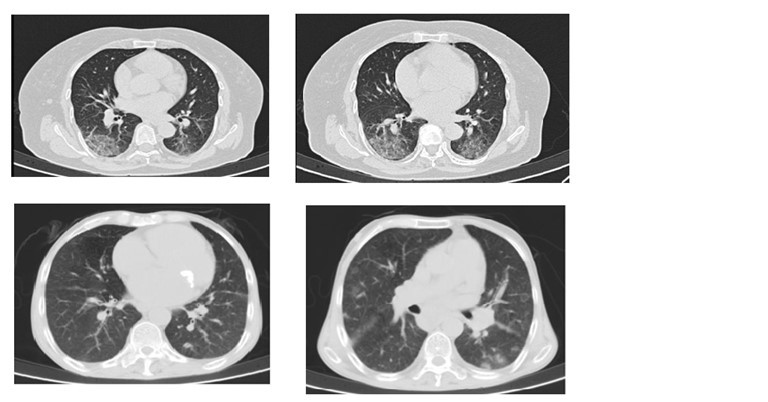
The most common CT findings in COVID-19 are ground glass opacities and consolidation noticed in 95% and 72% of the patients respectively. Ground glass opacities have been considered to be the result of serous inflammatory exudative reaction from lung alveoli. Copious amounts of such inflammatory exudation ultimately forms consolidation. Studies have reported prominent bilateral consolidation on CT scans in ICU patients. Ground-glass opacities and little areas of consolidations are seen in patients with mild symptoms of the infection not mounting to the admission.
Clinical implications of these findings are that manifestation of the disease in early stage are ground-glass opacities and as the severity progresses consolidation becomes eminent in wider areas. In other words, such changes are predictive of rising possibilities of critical complications like acute respiratory distress syndrome or acute lung injury.
In a retrospective study, authors found patients with initial negative RT-PCR having mostly ground glass opacities and small areas of consolidation as compared to patients with positive initial RT-PCR results. Patients with mild lung injury as suggested by smaller consolidation areas on CT scan are having higher chances of getting negative initial RT-PCR result.
Role of CO-RADS score in COVID-19 diagnosis
CO-RADS (COVID-19 Reporting and Data System) scoring system was developed by the Dutch Association for Radiology. Grading can be used to assess the probability of COVID-19 lung Involvement. It is essential to consider the combination of patient’s exposure history, clinical symptoms, typical CT findings to recognise COVID-19 with higher sensitivity.
Referring to RT-PCR as standard, the specificity, sensitivity and accuracy of chest CT were 25%, 97% and 68% respectively in suggesting COVID-19 infection. The negative predictive value was 83% and the positive predictive value was 65%. (Tao Ai et al., Radiology 2020)
| Score | Interpretation |
| CO-RADS 0 | Uninterpretable: Scan technically insufficient for assigning a score |
| CO-RADS 1 | Very low probability: Normal or non-infectious |
| CO-RADS 2 | Llow: Typical for other infection but not COVID-19 |
| CO-RADS 3 |
Equivocal: Features compatible with COVID-19, but also other diseases |
| CO-RADS 4 | High: Suspicious for COVID-19 |
| CO-RADS 5 | Very high: Typical for COVID-19 |
| CO-RADS 6 | Proven: RTPCR positive for SARS-CoV-2 |
A recently published study of a predictive machine learning model by Hermans et al. showed that in addition to the CO-RADS score, other data parameters such as leucocyte count, creatine kinase, ferritin, diarrhoea as a symptom, and the number of days since onset of disease increased the prediction accuracy for COVID-19 infection.
Considering classical and characteristic COVID findings, CT proves its irreplaceable role in the diagnosis. It can be considered as an add on standard for COVID diagnosis in suspected patients in high prevalent areas and in those having negative RT PCR test.
Click here to see references
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author, Dr. Monish S Raut is a Consultant in Cardiothoracic Vascular Anaesthesiology. His area of expertise is perioperative management and echocardiography with numerous publications in various national and international indexed journals.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
