10 Things Nephrologists Wish All Doctors Knew
M3 India Newsdesk May 06, 2023
There are many things which a nephrologist takes into consideration while examining a patient. Listed here are the top 10 most important clinical pearls in the field of nephrology which will help you in your daily practice.
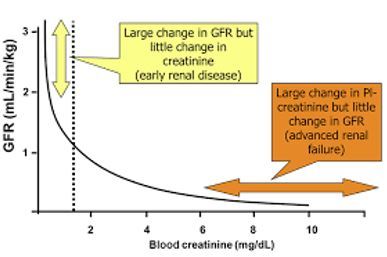
1. A “normal” serum creatinine level may not be normal
- Normal creatinine values may vary among different laboratories.
- The interpretation of serum creatinine level is affected by other factors like:
- Muscle mass
- Age
- Sex
- Height
- Limb amputation
- We have to always calculate eGFR with s.creatinine:
- Simple formula available freely online
- CKD-EPI ( Recommended by KDIGO)
- MDRD
- Cockcroft-gault formula
GFR and serum creatinine correlation
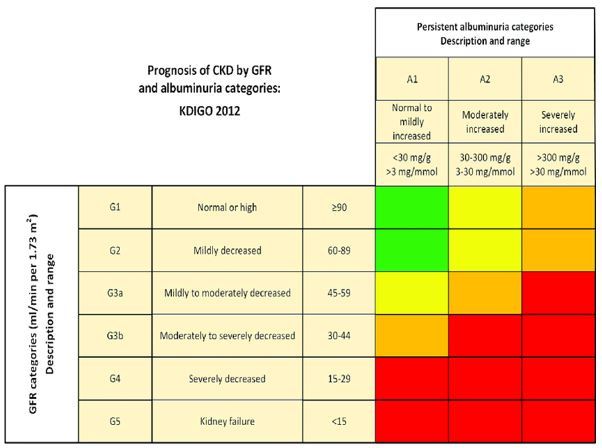
CKD stages- KDIGO classification
2. Screening for secondary hypertension, certain clinical clues may suggest reversible causes that might improve the patient’s hypertension
Clinical findings that may indicate secondary hypertension include:
- Hypertension that suddenly develops or suddenly worsens.
- Severe or difficult-to-control hypertension.
- Hypokalemia may suggest primary aldosteronism.
- Headaches, palpitations, and sweats may suggest pheochromocytoma.
- Moon faces, and/or striae may suggest Cushing syndrome.
- A history of snoring in an obese patient may suggest obstructive sleep apnoea.
- The deterioration of renal function or blood pressure after starting an ACEI or ARB could be an indication of the presence of renal artery stenosis.
Clinicians should interrogate regarding:
- Medications (NSAIDs, birth control pills, or certain decongestants)
- Lack of adherence to dietary restrictions (ingestion of sodium-containing foods)
- Review the patient’s anti-hypertensive drug regimen for appropriateness
3. Patients with decreased GFR or proteinuria should be evaluated to determine the cause
- A positive urine dipstick test for protein requires follow-up with a spot urine protein to urine creatinine ratio.
- The spot urine protein to creatinine ratio is a preferred method for accurately estimating protein excretion and is more convenient than a 24-hour urine collection.
- Patients with significant proteinuria or active urinary sediment, particularly with declining kidney function, should be referred to a nephrologist for additional assessment and management.
- Any patient with an elevated ratio (≥1) should be evaluated for causes of glomerular disease such as:
- Diabetes
- Collagen vascular disease (e.g., systemic lupus erythematosus)
- Malignancy (e.g., multiple myeloma)
- Infections (e.g., human immunodeficiency virus infection, syphilis, hepatitis B and C)
- Medications such as nonsteroidal anti-inflammatory drugs (NSAIDs)
4. Periodic evaluation and intervention in early-stage CKD
- To prevent complications and slow the advancement of renal disease, patients with early-stage CKD require periodic assessment and intervention.
- ACEIs and ARBs are effective in reducing the progression of CKD, particularly in individuals with proteinuria.
- Renal osteodystrophy is a potential risk in patients with progressive CKD, and close monitoring of phosphorus, calcium, and parathyroid hormone levels is necessary, especially in those with stage 3 to 4 CKD.
- Patients with CKD also have an increased risk of cardiovascular complications, including myocardial infarction and aggressive lipid-lowering strategies should be used like statins, with a goal low-density lipoprotein cholesterol (LDL-C) level of 100 mg/dL or less.
5. Do not automatically discontinue an ACEI or ARB solely because of a small increase in the serum creatinine or potassium level
- ACE-I/ARB are drugs of choice to prevent the progression of proteinuric CKD.
- Patients who begin taking or have a dose increase in ACEIs or ARBs may experience an increase in the serum creatinine level. Although an increase of 20% to 30% is acceptable.
- Follow-up serum creatinine and potassium levels should be obtained within a week.
- If the creatinine level increases by more than 20-30% or hyperkalemia cannot be controlled, the ACEI or ARB dose should be reduced or discontinued.
6. Anaemia in patients with CKD should be treated with erythrocyte-stimulating agents, such as recombinant human erythropoietin, but should not be over-treated
- KDOQI guideline for the treatment of anaemia of CKD recommends that the haemoglobin target should be between 11 and 12 g/dL.
- Erythropoietin should be discontinued in patients with a haemoglobin level of 13 g/dL.
- All patients with anaemia should be evaluated for other reversible causes, including vitamin deficiencies and iron deficiency.
- The iron deficiency must be corrected if erythrocyte-stimulating agents are to be effective.
7. In patients with recurrent stone disease, an in-depth metabolic evaluation is needed to identify and treat modifiable risk factors for preventing further episodes and/or promoting stone dissolution
Which patients should be referred to a nephrologist for further evaluation:
- Patients with a family history of stones
- Concomitant gastrointestinal diseases such as inflammatory bowel disease
- Frequent urinary tract infections
- Recurrent stone formers
- Associated with renal dysfunction
Patients without these risk factors should have a simplified evaluation that includes:
- Dietary history
- Review of medications that can promote stone development
- Urinalysis
- The levels of serum electrolytes, calcium, phosphorous, and uric acid should be measured
- Urinary metabolic profile
8. Arteriovenous fistula should be created in stage 5 CKD patients to avoid central venous catheterisation and associated complications
- The most common arteriovenous fistula techniques include the radio cephalic fistula, brachiocephalic fistula, and transposed brachiobasilic fistula.
- It is important to avoid inadvertent pricks in these veins during sampling and for intravenous cannulation.
9. Diagnose and intervene early in acute kidney injury
- Early diagnosis by simple measures of monitoring for urine output and getting serum creatinine reports
- Adequate hydration, maintenance of adequate circulating blood volume and mean arterial pressure, and avoidance of nephrotoxin
- Early apt nephrologist consultation to address any potentially reversible cause
- Indications for hemodialysis in AKI:
- Worsening severe metabolic acidosis
- Refractory pulmonary oedema
- Refractory hyperkalemia
- Uremic encephalopathy or pericarditis
- Certain drug intoxication
10. Dose modification for drugs having renal clearance
- Many drugs will need adjustment of dosages to avoid systemic toxicity.
- Judicious use of NSAIDS and aminoglycoside.
- Avoid phosphate-containing bowel enema in CKD to prevent phosphate nephropathy.
An additional point to note:
Cyclosporine and tacrolimus- Drugs commonly used in patients with renal transplants have many drug-drug interactions.
Case study 1
A 66-year-old man having hypertension has the following reports had a serum creatinine level of 0.8 mg/dL which had increased recently to 1.4mg/dL after taking some OTC medications. Hence his eGFR dropped from 103 to 54 mL/min per 1.73 m2 with just a 0.6mg/dl of creatinine increase.
Examination
On review, it was found that he was on ARB and had taken NSAIDs due to which his s.creatinine had increased.
Explanation
NSAIDS cause afferent artery constriction in the glomerulus whereas ARB causes post-glomerular efferent artery vasoconstriction. Hence it might lead to severe AKI.
Case study 2
A 60-year-old female presented to OPD with complaints of pedal oedema, joint pain and generalised weakness of 2 weeks duration, dry cough and dyspnoea on exertion of 5 days duration.
Blood reports
- S.creat-5.8 (1.45-->2.24-->5.8)
- Na+/K+- 143/3.2
- Hb -10.3 / TC -10,100 / PC- 284,000
Urine examination
- Protein 2+
- RBC 30-50
- Urine protein creatinine ratio 3769.75 mg/gm
Immunological tests
- ANA: Weak positive
- c-ANCA (MPO) positive
Renal Biopsy: Pauciimmune crescentic glomerulonephritis
Treatment
- She was treated with cyclophosphamide and steroids.
- A total of 3 cycles of cyclophosphamide were given at an interval of 3 weeks.
- Her s.creatinine was reduced to 1.4mg/dl and UPCR-560mg/gm.
- She is currently on low-dose steroids.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr. Bhavin Mandowara is a practising nephrologist at Zydus Hospital, Ahmedabad.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
