Treating Hypertension in General Practice
M3 India Newsdesk May 10, 2024
Hypertension is a silent killer. The burden has decreased because of awareness and prevention for about three decades. This article discusses the drugs used in HTN along with the characteristic features of these drugs. It also elucidates the role of diuretics in HTN.
Hypertension
When we think of treating hypertension the following points should be noted:
- At present because of lifestyle modifications, regular BP checks at least at home should be carried out for the first time at least 5 times a day for about a week and the average should be taken or it should be below 130/80mm Hg in most of the readings.
- Cutting off extra salt and salt-containing foods & walking 2 hrs a day (can be split) and back walking (at least 5 to 7 times) with good hydration decreases systolic by about 8 mm Hg.
- With any small symptoms like blacking out, fatigue, giddiness, age, family history, or obesity the person who visits the clinic should be made aware and BP should be recorded. If found below 120-130/80, with no other co-morbid conditions the patient should be made aware that he should get regular check-ups once in 3 months. If not at least bimonthly from the age of 20-25 (now because of LSM) to prevent having BP or to prevent complications like CCF, CKD etc.
- Once after recording for a week and coming to a conclusion that the person is hypertensive, counsel about the LSM once again and about the drugs which have to be taken regularly and continuously, and at proper times (follow chronotherapeutics) to maintain 24-hour suppression (physiologically) and hence can lead a life independently until death.
Drug treatment for hypertension
A brief drug treatment of HTN is given below:
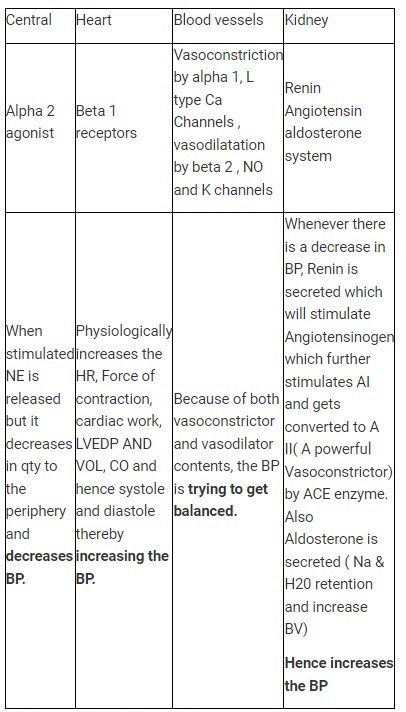
Physiological centres to maintain BP
The physiological balance should be understood before starting the drug treatment apart from age and other specifications.
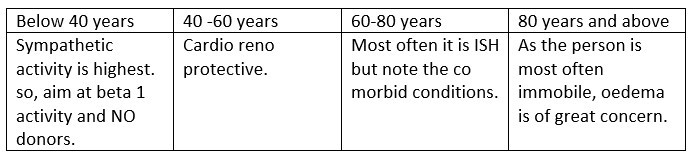
Age-related factors for HTN
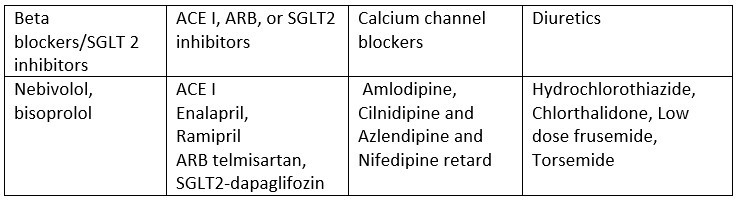
Based on the above criteria, we preferably choose the drugs as follows for hypertension per se:
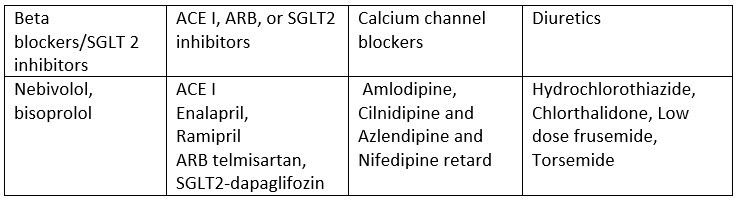
The above are the practice points for a newly diagnosed hypertensive patient. If there are co-morbid conditions, follow JNC-8 guidelines or A, B, C or D to treat them accordingly.
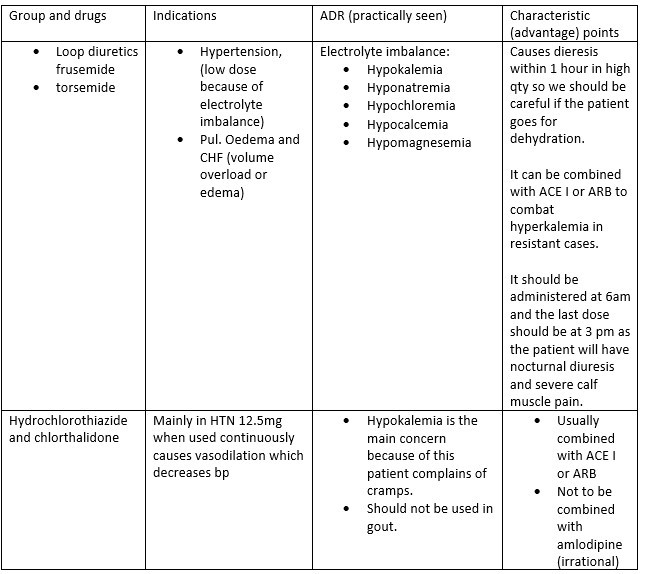
Characteristic features of the drug used in HTN
If the dose exceeds 80mg of telmisartan or 10mg of ramipril then combination therapy is preferred.
Diuretics in hypertension
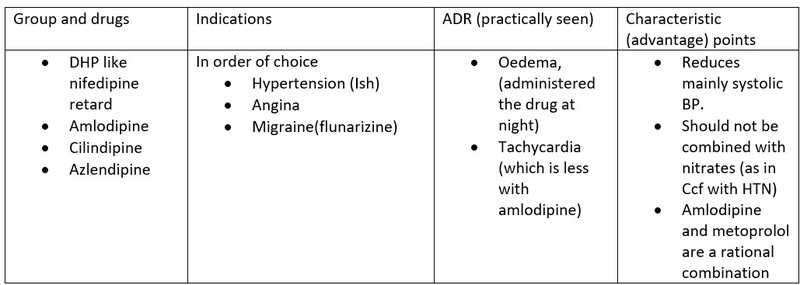
Calcium channel blockers
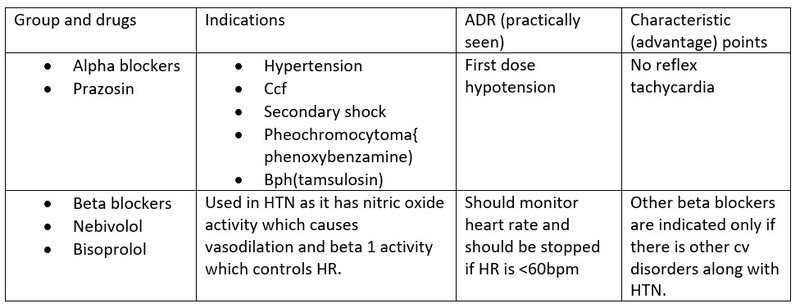
Adrenergic blockers (alpha and beta blockers)
Alpha-blockers are the choice when there is resistant hypertension (not able to control BP with combination therapy).
Beta-blockers are not the first drug of choice in HTN per se, however, it is the first choice in young hypertensives as there is a sympathomimetic drive.
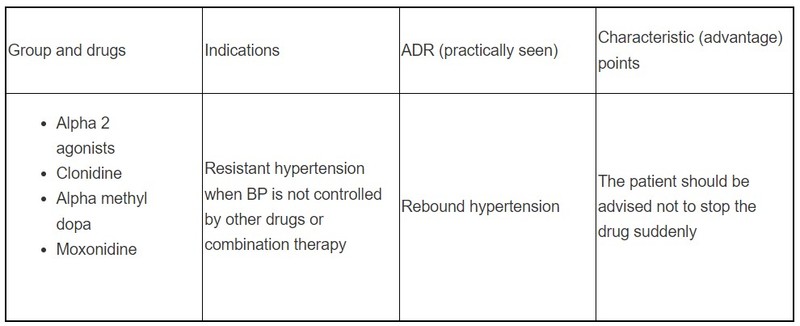
Centrally acting alpha 2 agonists
These are used only in resistant cases as there are side effects.
Pregnancy-induced hypertension
When bp is more than 120/80mmhg after 24 weeks of pregnancy then we call it pregnancy-induced hypertension (PIH). The drugs used are labetalol, amlodipine, alpha-methyl dopa, and hydralazine.
Combination therapy is preferred as it can target different areas and also lessen the side effects as the patient might not visit regularly.
Take-home message
- HTN is one of the major health problems that need a vigorous preventive and therapeutic approach including much more attention to detecting and treating hypertension at an earlier age.
- The choice of agents is ACE I, ARBs, CCB-DHP, and diuretics. ACEI or ARBs are chosen as they decrease morbidity (suffering).
- The combination of ACEI and Amlodipine or ACEI + diuretics should be the initial choice to have cardiorenoprotective mechanisms.
- Compliance should be of main concern as HTN is asymptomatic. Counsel regarding adherence to therapy. Regular visits for check-ups or home-based monitoring.
- FDC or polypill may be considered for compliance as it reduces the burden of taking it multiple times.
- In elderly, prefer diuretics and CCB as their initial choice.
- Check for blood lipids and target organ damage.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Padma Lakshminarayana is a professor and HOD of pharmacology at Sapthagiri Institute of Medical Sciences and Research Centre in Bengaluru.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
